Scapholunate advanced collapse (SLAC) of the wrist is the most common pattern of degenerative arthritis in the wrist. Watson and Ballet coined the term SLAC wrist in 1984.[1] Findings of bilateral SLAC wrist on a prehistoric skeleton from Hassi-el-Abiod site in Malian Sahara provide paleopathological evidence of the existence of this disease 7000 years ago.
An image depicting scapholunate advanced collapse can be seen below.
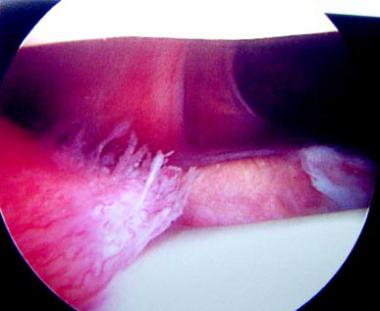
 Stage 2 scapholunate advanced collapse (SLAC) wrist. Next
Stage 2 scapholunate advanced collapse (SLAC) wrist. NextThe hallmark of scapholunate advanced collapse (SLAC) is scaphoid or scapholunate ligament injury with collapse on the radial side of the wrist.
Scapholunate advanced collapse (SLAC) has been reported to be more common in men than in women and more common in persons who perform manual labor than in other individuals. It is most common in the dominant wrist. SLAC has been reported in people aged 19-82 years. The peak decade for corrective SLAC surgery is the fourth decade of life. The periscaphoid area is the site of 95% of all wrist degenerative diseases. The SLAC pattern is seen in 57% of patients with periscaphoid arthritis.
A scapholunate advanced collapse (SLAC) wrist pattern is the result of many radial-sided wrist pathologies (see the images below). Most common is scapholunate dissociation with rotatory subluxation of the scaphoid. Scaphoid nonunion advanced collapse (SNAC) is another very common cause.[2]
Stage 2 scapholunate advanced collapse (SLAC) wrist.  Scapholunate advanced collapse (SLAC) wrist from nonunion of the scaphoid. The patient underwent 4-bone fusion.
Scapholunate advanced collapse (SLAC) wrist from nonunion of the scaphoid. The patient underwent 4-bone fusion.  Scapholunate advanced collapse (SLAC) wrist from nonunion of the scaphoid. The patient underwent 4-bone fusion.
Scapholunate advanced collapse (SLAC) wrist from nonunion of the scaphoid. The patient underwent 4-bone fusion. Other etiologies include Preiser disease (avascular necrosis of the scaphoid),[3] midcarpal instability, intra-articular fractures involving the radioscaphoid or capitate-lunate joints, Kienböck disease (see the image below),[4] primary degenerative arthritis with attenuation of the scapholunate ligament and scapholunate dissociation,[5, 6] capitolunate degeneration, and inflammatory arthritis, such as seen in the crystalline deposition disorders of gout and calcium pyrophosphate dihydrate deposition disease (CPPD).[7, 8]
 Scapholunate advanced collapse (SLAC) wrist from Kienböck disease.
Scapholunate advanced collapse (SLAC) wrist from Kienböck disease. Initial treatment of the cause of the SLAC wrist (eg, scaphoid nonunion, scapholunate dissociation) may prevent subsequent degeneration.
The distal radius has 2 articular fossae for the scaphoid and lunate. The scaphoid fossa is elliptical or ovoid. It narrows toward the radial styloid in a dorsal-volar plane. Thus, the scaphoid proximal articular surface is shaped like a spoon. The lunate fossa is spherical. Injury of the scaphoid or its supportive ligaments can cause radial-sided collapse with flexion of the scaphoid, thus resulting in incongruence of the radioscaphoid joint.
Thus, narrowing of the radioscaphoid joint first begins at the radial styloid aspect (stage 1A). Radiographic changes appear as a sharp elongation on the radial styloid. As the disease progresses, the rest of the radioscaphoid joint is destroyed (stage 1B). In stage 1B, the entire scaphoid fossa is involved. Complete collapse of radioscaphoid joint alters the normal load-bearing ability of the capitolunate joint. This results in a radial or dorsal radial position of the capitate. Shear stress destroys cartilage in the capitolunate joint leading to the most advanced stage, midcarpal scapholunate advanced collapse (SLAC) (stage 2). In stage 2, the capitolunate joint is additionally narrowed and sclerotic. As the arthritic pattern thus progresses, it shifts from the scaphoid fossa of the radius to the midcarpal capitate articulation.
At all stages of SLAC wrist, the radiolunate joint is not involved because of its spherical shape. The lunate is congruently loaded in every position and, thus, highly resistant to degenerative changes. This sparing of the lunate fossa provides a basis for some of the motion-preserving procedures to treat SLAC wrist. Long-standing and untreated SLAC wrist can lead to a painful wrist at rest and during use, deterioration of range of motion (ROM), and decreased grip strength. The radiographic SLAC appearance does not always correlate with the patient's symptoms.
A history of wrist injury, scaphoid fracture, carpal tunnel decompression, or carpal ganglion excision may be present. Many patients with scapholunate advanced collapse (SLAC) wrist have minimal symptoms and may present because of a secondary problem, such as carpal tunnel syndrome. Patients may have a variable duration history of wrist pain during activity. Patients relate their symptoms to increased activity and overuse. Postactivity pain may be present. Patients may have modified their activities, depending on the severity of symptoms. Many patients have used nonsteroidal anti-inflammatory drugs (NSAIDs) for pain relief.
Wrist edema may be present, and patients may have pain with motion, especially when loading the wrist in an extended position. Limited wrist ROM is typical, and an average wrist flexion/extension arc of 80-90° has been reported. Direct palpation of the scapholunate joint or radiocarpal joint generally elicits pain. Pain with resistance against active finger extension while the wrist is held in passive flexion is common. A scaphoid shift test also elicits pain. To perform this maneuver, the examiner places the fingers of the same hand on the dorsum of the distal radius of the wrist being examined (ie, the left hand is used to examine left wrist). The examiner's thumb is placed volarly on the scaphoid tuberosity and pushed dorsally while passively radially and ulnarly deviating the patient's wrist with the other hand. This stresses the periscaphoid ligaments and subluxes the scaphoid dorsally, thus eliciting pain if periscaphoid disease is present.
Differential clinical diagnoses of SLAC wrist arthritis include essentially any condition that causes dorsal radial wrist pain. Common differential diagnoses include scaphoid fractures, de Quervain tenosynovitis, scapholunate dissociation, Kienböck disease, distal radial fracture, Preiser disease, and scaphotrapezoid-trapezial (STT) joint arthritis.
Asymptomatic scapholunate advanced collapse (SLAC) wrist generally does not require treatment, although some patients may require surgery for secondary problems, such as carpal tunnel syndrome. Mild symptomatic SLAC can often be managed nonoperatively. For more symptomatic SLAC, operative intervention is warranted. The surgical procedure is planned based on radiographic findings, symptoms, physical examination findings, and the surgeon's preference. Since more motion occurs at the radiocarpal joint than the midcarpal joint, and since the radiolunate joint is generally spared, a limited wrist fusion with scaphoid excision is an option, although a total wrist fusion is often more predictable in alleviating pain. In stage 1 SLAC with sparing of the capitolunate joint, a proximal row carpectomy (PRC) may also be used to preserve partial wrist motion.
See Surgical therapy.
See Surgical therapy.
Workup
Copyright © www.orthopaedics.win Bone Health All Rights Reserved