What is now known as a triplane fracture is believed to have first been reported in 1957 by Johnson and Fahl.[1] Ehalt, in 1961, and Titze, in 1967, described similar fractures of the distal lateral tibia and tibial epiphysis as transitional fractures.[2, 3]
In 1970, Marmor first described a fracture that involved the distal tibia and distal tibial epiphysis as having three separate fragments, including the anterolateral distal tibial epiphysis, the anteromedial and posterior portions of the distal tibial epiphysis with an attached posteromedial spike of the distal tibial metaphysis, and the remainder of the distal tibial metaphysis and shaft.[4] This fracture pattern was recognized to have fracture lines in the transverse, coronal, and sagittal anatomic planes.
In 1972, Lynn first coined the term triplane fracture in his paper describing the reduction surgery in two patients with distal tibial epiphyseal injuries, both of whom had fractures in the sagittal, coronal, and transverse planes.[5] In 1978, Cooperman reviewed 237 cases of distal tibial epiphyseal fractures. Fifteen (6%) were triplane fractures, of which 13 were treated by closed reduction.[6]
In 1981, Denton and Fischer reported a triplane fracture that was unusual in that it was a medial triplane fracture.[7] Von Laer and, later, Etrl continued investigations into the nature of the tibial triplane fracture.[8, 9]
A triplane fracture of the distal tibia is generally sustained during adolescence and occurs before complete closure of the distal tibial physis (growth plate). It represents 5-10% of pediatric intra-articular ankle injuries and typically presents in children aged 12-15 years. The incidence is slightly higher in boys than in girls.[10, 11, 12, 13, 14, 15, 16]
The characteristic asymmetric closure of the distal tibial growth plate occurring over a period of approximately 18 months is the basis for the unique occurrence of this fracture following an ankle injury in this age group.
The classic fracture pattern is multiplanar. The fracture extends through the transverse (growth plate), sagittal (epiphysis), and coronal (distal tibial metaphysis) anatomic planes, disrupting the tibial plafond intra-articularly, resulting in three classically described fragments. It has, however, several variations.
Some practitioners prefer to call the fracture an adolescent tibial triplane fracture because this term is more descriptive of the age of occurrence, location, and fracture pattern. It is also termed transitional injury because it occurs during the period of transition from skeletal immaturity to skeletal maturity.
Articular congruity at the ankle joint surface, not physeal arrest or growth retardation, is the major concern with triplane fractures. Therefore, nondisplaced fractures and extra-articular fractures can be managed nonoperatively, but displaced fractures require anatomic reduction and internal fixation. Malunited fractures with over 2 mm of intra-articular displacement are associated with poor outcomes.
For patient education resources, see the First Aid and Injuries Center, as well as Ankle Fracture.
NextTriplane fracture of the ankle involves the bony structures and their associated ligamentous supports (see the image below).
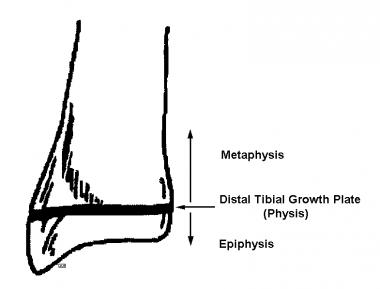 Triplane fracture involves the tibial metaphysis, tibial growth plate (physis), and the epiphysis. This image depicts each of the involved anatomic areas. It is important to recall the structural lines of development and maturation of the metaphysis, physis, and epiphysis, as they relate to the triplane fracture. Note that forces transmitted to the physis and epiphysis create fracture lines consistent with the maturity of these structures. For an unfused growth plate, separation is likely to occur here. When the growth plate is fused (closed), the avulsed portion is likely the most recent portion of the growth plate that has fused. This part represents the weakest (least calcified and least matured) portion of the physis. Frequently this involves the anterolateral growth plate.
Triplane fracture involves the tibial metaphysis, tibial growth plate (physis), and the epiphysis. This image depicts each of the involved anatomic areas. It is important to recall the structural lines of development and maturation of the metaphysis, physis, and epiphysis, as they relate to the triplane fracture. Note that forces transmitted to the physis and epiphysis create fracture lines consistent with the maturity of these structures. For an unfused growth plate, separation is likely to occur here. When the growth plate is fused (closed), the avulsed portion is likely the most recent portion of the growth plate that has fused. This part represents the weakest (least calcified and least matured) portion of the physis. Frequently this involves the anterolateral growth plate.
The tibia is the main weightbearing bone of the lower leg. The tibial metaphysis consists of the distal quarter of the tibia, excluding the tibial growth plate and epiphysis.
The distal tibial physis, also called the growth plate, is located between the tibial metaphysis and the epiphysis. The distal tibial epiphysis is bordered proximally by the physeal growth plate and distally by its articulation with the articular surface of the talar dome. It contributes 50% of tibial growth and approximately 4-6 mm (0.25 in.) of longitudinal growth per year.[17, 18]
The fibula is situated laterally along the length of the tibia in the lower leg, giving stability to the lateral ankle joint and serving in a nonweightbearing role.
The ankle joint bears more weight per unit surface area than any other joint in the body. The ankle joint is formed by the fibula (laterally), the tibia (superiorly and medially), and the dome of the talus (inferiorly). The joint is saddle-shaped. The dome of the talus becomes wider anteriorly, such that when the foot is in dorsiflexion, the talus is situated more snugly in the tibiofibular saddle than when the foot is plantarflexed. Thus, plantarflexion (a position contributing to the triplane fracture) is a less stable position of the ankle than is dorsiflexion.
The only pure motions of the ankle joint are dorsiflexion and plantarflexion. Inversion and eversion of the ankle joint take place at the subtalar joint formed by the opposition of the talus and the inferiorly situated calcaneus. The talus always moves in the same direction as the calcaneus in normal gait.
Ankle injuries typically follow forces that are directed perpendicularly (inversion or eversion) to the normal motion of the ankle. That motion is perpendicular to the motions of dorsiflexion and plantarflexion that occur in the sagittal plane.
Ligamentous support of the ankle is extensive. Ligaments situated laterally consist of anterior and posterior talofibular and tibiofibular ligaments. The strong deltoid ligament is located medially and is the only ligament of the ankle containing elastic fibers.
The tibia and fibula are joined by the anterior and posterior talofibular ligaments distally and the interosseous membrane more proximally.
Knowledge of the anatomic planes of the body is essential to understanding the lines, planes, and fragments produced in a triplane fracture. In the anatomic position (ie, with the person standing, palms forward), these two-dimensional planes are as follows:
Motions of the ankle and foot are described by a number of interchangeable terms, including the following:
Neurovascular structures in the area of the ankle and foot include the following:
Triplane fracture of the distal tibia rarely occurs outside of adolescence. This is directly related to the pattern of distal tibial growth plate closure as skeletal maturity is attained (see the image below).
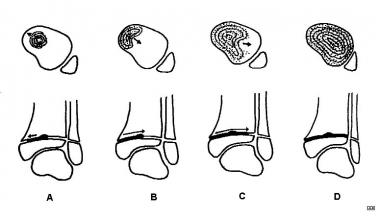 (A) The distal tibial growth plate begins to close with a centrally located epiphyseal hump and proceeds medially, with posterior closure occurring before anterior closure. Following medial closure, the lateral tibial growth plate then closes progressively from the posteromedial area (B) to the anterolateral area (C, D). The entire process of physeal closure usually spans a period of 18 months. This process generally occurs when the individual is aged 12-15 years (mean age is 13.5 years, age range is 10-18 years), with complete closure occurring earlier in girls than in boys.
(A) The distal tibial growth plate begins to close with a centrally located epiphyseal hump and proceeds medially, with posterior closure occurring before anterior closure. Following medial closure, the lateral tibial growth plate then closes progressively from the posteromedial area (B) to the anterolateral area (C, D). The entire process of physeal closure usually spans a period of 18 months. This process generally occurs when the individual is aged 12-15 years (mean age is 13.5 years, age range is 10-18 years), with complete closure occurring earlier in girls than in boys.
The distal tibial epiphysis begins to close with a centrally located epiphyseal hump and proceeds medially, with posterior closure occurring before anterior closure. Adolescent children are susceptible to a triplane fracture after medial physeal closure and before lateral physeal closure. After medial closure, the lateral tibial growth plate closes progressively from the posteromedial area to the anterolateral area. The anteromedial tibial growth plate is the last area to close; therefore, it is more prone to injury than any other area of the tibial growth plate.
The entire process of distal tibial growth plate closure (physiologic epiphysiodesis) usually spans a period of 18 months. This process generally occurs when the individual is aged 12-15 years (mean age, 13.5 years), with complete closure occurring earlier in girls than in boys.
Regardless of the age of the patient, it is important to remember that variation (age range, 10-18 years) exists around the mean age of expected closure of the tibial growth plate. Any time the lateral distal tibial growth plate is open (unfused), the patient is susceptible to a triplane fracture.
As previously described, a triplane fracture involves fracture lines in the sagittal, coronal, and transverse planes; however, there are three types of triplane fractures, as follows:
Each type may have a coexisting fibular fracture as well, but this is not counted as a component of the triplane fracture; only tibial fragments are counted as such. Other rare and unusual variants of the two- and three-part triplane fractures have been reported, such as the medial triplane fracture described by Denton and the triplane fracture shown in the images below.[7]
 Lateral radiograph of a triplane fracture illustrates the following: Yellow arrows indicate the horizontal component of the fracture through the physis (growth plate), red arrows indicate the vertical fracture line in the coronal plane involving the metaphyseal spike complex, black arrows point to the posterior margin of the metaphyseal spike, and purple arrows indicate the associated fibular fracture. This image represents one of the first known published images of this type of 2-part triplane fracture.
Lateral radiograph of a triplane fracture illustrates the following: Yellow arrows indicate the horizontal component of the fracture through the physis (growth plate), red arrows indicate the vertical fracture line in the coronal plane involving the metaphyseal spike complex, black arrows point to the posterior margin of the metaphyseal spike, and purple arrows indicate the associated fibular fracture. This image represents one of the first known published images of this type of 2-part triplane fracture.
 Radiograph of a triplane fracture. The anterior-posterior view of the distal tibia and epiphysis is illustrated as follows: Yellow arrows indicate the horizontal fracture component through the growth plate, white arrows indicate the vertical fracture through the epiphysis in the sagittal plane, and black arrows outline the superior edges of the posterior metaphyseal spike. An associated fibula fracture is present. In this left-sided 2-part triplane fracture, medial is to the viewer's left, and lateral is to the right. This image represents one of the first known published images of this type of 2-part triplane fracture.
Radiograph of a triplane fracture. The anterior-posterior view of the distal tibia and epiphysis is illustrated as follows: Yellow arrows indicate the horizontal fracture component through the growth plate, white arrows indicate the vertical fracture through the epiphysis in the sagittal plane, and black arrows outline the superior edges of the posterior metaphyseal spike. An associated fibula fracture is present. In this left-sided 2-part triplane fracture, medial is to the viewer's left, and lateral is to the right. This image represents one of the first known published images of this type of 2-part triplane fracture.
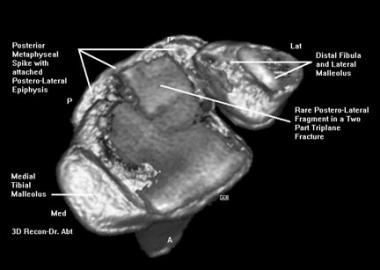 Digital 3-dimensional helical CT scan reconstruction of a rare type of triplane fracture. The image shown is of the inferior surface of the tibial epiphysis. Medially (viewer's left) is the distal tibial malleolus. Laterally (viewer's right) is the distal fibula/lateral malleolus. Fracture lines exist through the tibial epiphysis in the coronal, sagittal, and horizontal planes. The posterolateral fragment of the epiphysis is attached to the posterior metaphyseal spike rather than the more common anterolateral segment of the epiphysis. This image represents one of the first known published images of this type of 2-part triplane fracture.
Digital 3-dimensional helical CT scan reconstruction of a rare type of triplane fracture. The image shown is of the inferior surface of the tibial epiphysis. Medially (viewer's left) is the distal tibial malleolus. Laterally (viewer's right) is the distal fibula/lateral malleolus. Fracture lines exist through the tibial epiphysis in the coronal, sagittal, and horizontal planes. The posterolateral fragment of the epiphysis is attached to the posterior metaphyseal spike rather than the more common anterolateral segment of the epiphysis. This image represents one of the first known published images of this type of 2-part triplane fracture.
 Two-dimensional helical CT scan image prior to 3-dimensional reconstruction. PLEF represents the posterolateral epiphyseal fragment. DF is the distal fibula. The posteromedial and the entire portion of the anterior epiphysis are intact. This image represents one of the first known published images of this type of 2-part triplane fracture.
Two-dimensional helical CT scan image prior to 3-dimensional reconstruction. PLEF represents the posterolateral epiphyseal fragment. DF is the distal fibula. The posteromedial and the entire portion of the anterior epiphysis are intact. This image represents one of the first known published images of this type of 2-part triplane fracture.
In a two-part triplane fracture (see the image below), the first fracture line in the transverse (horizontal) plane is through the tibial epiphysis, leaving the anteromedial portion of the epiphysis attached to the distal tibia. The second fracture line is in the sagittal plane through the epiphysis, lateral to the original formation of the epiphyseal fusion hump. The third fracture line is in the coronal plane and courses superiorly through the posterior metaphysis, producing a posterior metaphyseal spike. The following two fragments result:
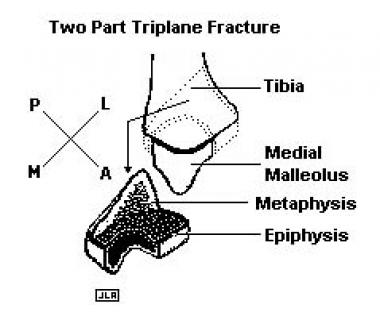 In a 2-part triplane fracture, 3 fracture lines are identified in each of the transverse, coronal, and sagittal planes. The first fracture line in the transverse (horizontal) plane is through the growth plate (physis), leaving the anteromedial portion of the physis attached to the distal tibia. The second fracture line is in the sagittal (anteroposterior) plane through the epiphysis, lateral to the original formation of the epiphyseal fusion hump. The third fracture line is in the coronal plane and courses superiorly through the posterior metaphysis, producing a posterior metaphyseal spike. The resulting 2 fragments are (1) a fragment consisting of the posteromedial and lateral portions of the epiphysis attached to a posterior metaphyseal spike and (2) the distal tibia, with the anteromedial epiphysis attached.
In a 2-part triplane fracture, 3 fracture lines are identified in each of the transverse, coronal, and sagittal planes. The first fracture line in the transverse (horizontal) plane is through the growth plate (physis), leaving the anteromedial portion of the physis attached to the distal tibia. The second fracture line is in the sagittal (anteroposterior) plane through the epiphysis, lateral to the original formation of the epiphyseal fusion hump. The third fracture line is in the coronal plane and courses superiorly through the posterior metaphysis, producing a posterior metaphyseal spike. The resulting 2 fragments are (1) a fragment consisting of the posteromedial and lateral portions of the epiphysis attached to a posterior metaphyseal spike and (2) the distal tibia, with the anteromedial epiphysis attached.
In a three-part triplane fracture (see the image below), three fracture lines again are present in each of the three anatomic planes; however, the fracture line in the coronal plane is complete in its course through the epiphysis, as well as through the posterior metaphysis. The following three fracture fragments are produced:
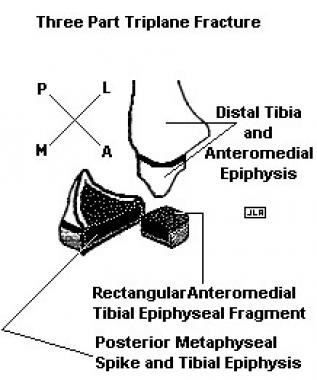 In a 3-part triplane fracture, the 3 fracture lines are present in each of the 3 anatomic planes; however, the fracture line in the coronal plane is complete in its course through the epiphysis and posterior metaphysis. The 3 fracture fragments thus produced are (1) a rectangular fragment of the anterolateral portion of the epiphysis, (2) the remainder of the epiphysis with an attached posterior spike of the distal tibial metaphysis, and (3) the tibial shaft with the proximal metaphysis and anteromedial epiphysis.
In a 3-part triplane fracture, the 3 fracture lines are present in each of the 3 anatomic planes; however, the fracture line in the coronal plane is complete in its course through the epiphysis and posterior metaphysis. The 3 fracture fragments thus produced are (1) a rectangular fragment of the anterolateral portion of the epiphysis, (2) the remainder of the epiphysis with an attached posterior spike of the distal tibial metaphysis, and (3) the tibial shaft with the proximal metaphysis and anteromedial epiphysis.
The four-part triplane fracture is similar to the three-part fracture, with the exception that the fourth fragment consists of the medial malleolus. This is a result of the extension of the fracture forces projecting more medially in the horizontal plane.
Shin et al classified a subtype of triplane fractures in which the fracture extended into the medial malleolus.[19] Using three-dimensional (3D) computed tomography (CT), they delineated the intramalleolar fracture patterns and demonstrated three distinct types of intramalleolar triplane fractures, as follows:
A quadriplane fracture (ie, a typical triplane fracture plus a metaphyseal fragment) has been described. A combination of external rotation and vertical compression has been proposed as the mechanism of injury.[20]
Kleiger and Mankin described an elevation or hump in the growth plate, about 1 cm from its medial edge, in 40% of adolescents between the ages of 12 and 20 years. They suggested that the medial hump might prevent displacement of the medial part of the epiphysis by a rotational force.[21] This was corroborated by Clement and Worlock, who suggested that the medial hump may stabilize the anteromedial part of the epiphysis in the same way as fusion of the medial part of the plate in older children.[22]
Dias and Giegerich suggested that two grades of injury can result from a lateral or external rotation force applied to the distal tibia during the period of growth plate fusion. In a grade I injury, the anterior tibiofibular ligament avulses the anterolateral corner of the distal tibial epiphysis (the juvenile Tillaux fracture). The Tillaux fracture fragment in adults is virtually identical to the anterolateral epiphyseal fragment in a triplane fracture. If there is further lateral or external rotation, the remainder of the distal tibial epiphysis separates through the growth plate, taking with it an attached posteromedial metaphyseal fragment and producing a grade II three-part triplane fracture.[23]
Triplane fracture is the result of several factors that exist simultaneously, including the following:
Triplane fracture occurs most commonly in patients aged 12-15 years. It represents 5-10% of all pediatric intra-articular ankle injuries.
The male-to-female frequency ratio ranges from 1:1 to 2:1 in the literature. In studies indicating a higher incidence in males, this is postulated to be caused by later closure of the lateral tibial growth plate in males than in females, thereby lengthening the period of vulnerability to injury for males.
A higher incidence in the right ankle is reported most often. However, one report noted a preponderance in the left ankle.[24]
Two-part triplane fractures occur more commonly and at a younger age than 3-part triplane fractures. This reflects the fact that relatively less closure of the tibial epiphysis exists in the 3-part group than in the 2-part group.
Missed or incompletely diagnosed triplane fractures initially were evaluated with plain film radiography without further CT studies.
Of the 8683 childhood and adolescent fractures evaluated by Landin over a 9-year study period, 4% (373) were ankle fractures.[25] More than 50% of ankle injuries were sustained during a fall. Right-side injury predominated almost 2:1. Seasonally, over the 9-year study period, peak incidence was in April and September, with the lowest frequency in July and December. Males sustained more ankle fractures than did females. For males, the incidence for each of the 2-year age groups studied was highest for those aged 15-16 years. For females, incidence was highest for those aged 13-14 years. During the study period, the incidence of ankle injuries progressively increased. This may reflect the increasing popularity of roller skates, skateboards, and scooters.
Devalentine found upon review of 118 epiphyseal injuries in childhood that 25% involved the distal tibial or fibular epiphyses.[26] MacNealy studied 194 cases of injuries of the distal tibial epiphysis and reported that 9.8% were triplane fractures.[27] The fibula is fractured in approximately 50% of triplane fractures.[9, 28, 29]
Although other associated injuries are uncommon, ipsilateral tibial shaft fractures[30] and a Maisonneuve fracture[11] associated with a triplane ankle fracture have been described.
The outcome and long-term prognosis for individuals with triplane fracture are related primarily to concerns in the following two areas:
Intraoperatively, it is important not to place compression screws or other hardware that exert compression forces on the growth plate. Such compression exacerbates premature growth plate closure and tibial growth retardation. Also, any physeal gaps lead to bony bridge formation and therefore require perfect reduction.
Rotational malalignment, which most often manifests as external rotation deformity, will adversely affect the foot progression angle.[31]
Postoperative infection and osteomyelitis are uncommon complications. Either may be attributed to a lack of patient cleanliness and compliance or to poor surgical technique, or may result from a highly contaminated open fracture.
Pressure sores may result from localized swelling, a cast that gets wet and expands, or a cast that is fitted improperly. In all such cases, the patient develops point tenderness that was not present previously under the cast. Remove the cast, and inspect and palpate the entire area to identify the location and cause of the pain.
If the pain is caused by pressure alone, a new cast is applied with extra padding in the area of pain and attention to avoiding all pressure to the area. If a pressure sore (skin breakdown) is noted, standard wound therapy, which may include oral antibiotics, should be initiated. The cast is reapplied as above, with the addition of a cast window. This allows ongoing wound checks and dressing changes until the wound resolves, while avoiding frequent cast changes for wound care.
Fracture blisters are caused by blood accumulating under the skin in an area of swelling that accompanies a fracture. This can result in skin breakdown and ulceration. Care of fracture blisters is similar to that for pressure sores. It is imperative that no surgical therapy for the fracture, initial or delayed, should be attempted at a site with fracture blisters because of the high risk of wound complications in the affected area.
Compartment syndrome may affect any of the four compartments of the lower leg or the deep plantar compartment of the foot. This may manifest as pain or burning, which may be severe at rest or with passive dorsiflexion of the foot. Sensation is affected first, then motor function.
Commonly, the anterior tibial compartment is affected with resultant increasing compartment pressure on the superficial peroneal nerve, which results in heightened pain on passive motion of the toes followed by decreased sensation in the first and second webspaces of the toes. The foot and/or lower leg may be tense and hard. Compare findings with those of the unaffected limb. If compartment syndrome is confirmed by measurement of compartment pressures, immediate operative intervention is required.
Clinical Presentation
Copyright © www.orthopaedics.win Bone Health All Rights Reserved