Phemister provided the first description of fibrous cortical defect (FCD) in 1929. Sontag and Pyle reported a radiologic description in 1941, and in 1942, Jaffe and Lichtenstein described clinical and anatomic aspects and the natural history.[1, 2] See radiographs below.
 Plain radiograph demonstrating multiple fibrous cortical defects in multiple bones.
Plain radiograph demonstrating multiple fibrous cortical defects in multiple bones.
 Plain radiograph of fibrous cortical defect of the proximal tibia.
Plain radiograph of fibrous cortical defect of the proximal tibia.
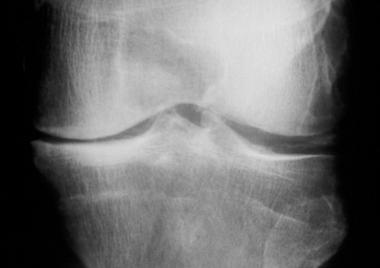
 Lateral radiograph demonstrating a solitary fibrous cortical defect in the proximal tibia.
Lateral radiograph demonstrating a solitary fibrous cortical defect in the proximal tibia.
Also called nonossifying or nonosteogenic fibroma, this benign tumor probably is the most frequent bony lesion in children, occurring in up to 30-40% of children.[3] The condition is most common in adolescents. Fibrous cortical defect is a term coined to describe the smaller variety of nonossifying fibromas.[4] However, no histologic difference exists between the lesions. When the lesion is large enough to encroach upon the medullary canal, the term nonossifying fibroma (NOF) is used. In this article, the terms FCD and NOF are interchangeable. The authors believe that these should be considered the same entity. These lesions are, in fact, developmental abnormalities, as opposed to benign neoplasms.
FCD usually is an incidental finding on radiographs. Always benign, these lesions may result in pathologic fracture, although pathologic fracture is a rare first presentation.[5] FCD can exist in multiple sites. FCD may be difficult to diagnose in the presence of pain or swelling of soft tissues. Fractures and impending fractures are indications for surgical intervention. Association with other bone lesions such as aneurysmal bone cyst is rare.[2, 4, 6, 7, 8, 9]
NextFibrous cortical defect (FCD) may present with a pathologic fracture, but this is an unusual presentation. FCD also can be confused with a more aggressive lesion. Therefore, biopsy may be necessary.
This lesion constitutes 5% of benign tumoral lesions of bone. The true incidence is more likely to be on the order of 30% or more, but because fibrous cortical defect (FCD) is asymptomatic in most patients, most lesions are never identified. Sontag and Pyle identified this lesion in 54% of boys and 22% of girls in a series of 200 healthy children.[3, 10] These lesions occur in multiple sites in approximately 50% of patients. This lesion is rare in children younger than 2 years and is most common in adolescents.
The etiology of fibrous cortical defect (FCD) remains obscure. FCD is a proliferation of benign fibrous tissue, possibly as a result of periosteal injury or secondary to abnormalities at the epiphyseal plate. Others postulate that FCD is related to the normal cutback phenomenon seen in maturing physeal plates. Progression of this lesion introduces abnormal tissue into the metaphyseal cortex.
The average duration of fibrous cortical defect (FCD) varies from 29-52 months, followed by spontaneous resolution. FCD may be present during childhood, but lesions tend to disappear in adolescence.
FCD is encountered frequently in children and adolescents and is usually asymptomatic.[3, 10, 11] Pain is rare and, if present, is usually associated with a fracture. Fibrous cortical defect (FCD) typically is localized in long bones. The most common sites are the femur and tibia. On rare occasions, it may be encountered in the vertebrae, clavicle, or bones of the upper limbs. The association of multiple FCDs with café au lait spots, multiple nevi, mental retardation, hypogonadism, and ocular and cardiovascular abnormalities is called Jaffe-Campanacci syndrome.[12]
FCD lesions have a typical and relatively distinct radiographic appearance. The lesion is radiolucent and is located eccentrically, usually in the distal metaphysis of a long bone. The cortex is thin, with sclerotic or scalloped margins. Lesions can be uniloculated or multiloculated. The longitudinal axis of FCD tends to be parallel to the axis of involved bone. Commonly, FCD can be diagnosed by the orthopedic surgeon on the basis of clinical findings and imaging, without need for referral to orthopedic oncology.[13]
The characteristic location and appearance are usually suggestive of a benign lesion and are often pathognomonic for fibrous cortical defect (FCD); thus, no further action is necessary unless a pathologic fracture has occurred or risk of fracture is high.
The following considerations should be kept in mind:
In the pediatric population, casting usually is the most appropriate treatment after pathologic fracture to avoid injuring the physes during surgery.[3] FCD may heal spontaneously following fracture. If, after casting and union of the fracture, the lesion does not regress, curettage and grafting are indicated. In unstable fractures or in adolescents, curettage (with or without grafting) and internal fixation are appropriate.
See Intraoperative details.
When fibrous cortical defect (FCD) is near an open physis, surgery should be avoided if possible. With time, the FCD will migrate away from the physis, and risk of damage to the growth plate will be minimized.
Workup
Copyright © www.orthopaedics.win Bone Health All Rights Reserved