Lateral epicondylitis, or tennis elbow, is a commonly encountered problem in orthopedic practice.
NextThe first description of lateral epicondylitis (tennis elbow) generally is attributed to Runge in 1873. Since this initial report, much controversy over the pathophysiology and treatment of this disorder has existed.
Lateral epicondylitis (tennis elbow) is an overuse injury involving the extensor muscles that originate on the lateral epicondylar region of the distal humerus. It is more properly termed a tendinosis that specifically involves the origin of the extensor carpi radialis brevis (ECRB).[1, 2, 3, 4] (See the images below.)
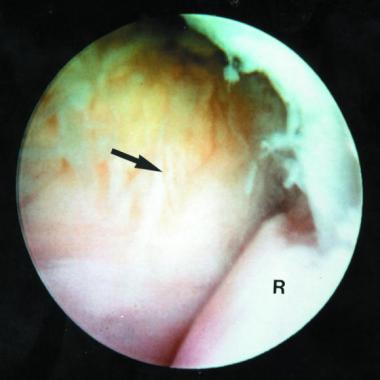 Type I lateral epicondylitis seen through the 30° arthroscope.
Type I lateral epicondylitis seen through the 30° arthroscope. 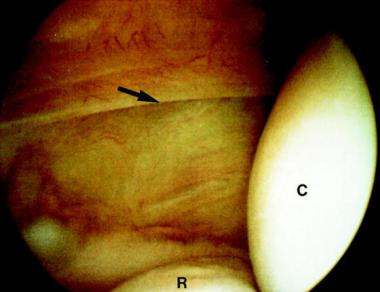 Type 2 lateral epicondylitis showing a linear tear in the origin of the extensor carpi radialis brevis muscle.
Type 2 lateral epicondylitis showing a linear tear in the origin of the extensor carpi radialis brevis muscle. 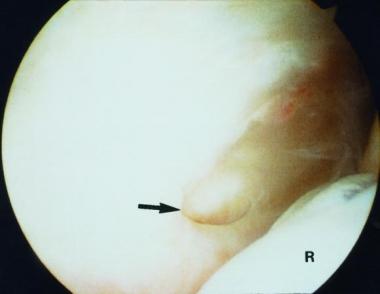 Type 3 lateral epicondylitis showing a large tear in the origin of the extensor carpi radialis brevis muscle.
Type 3 lateral epicondylitis showing a large tear in the origin of the extensor carpi radialis brevis muscle. Lateral epicondylitis (tennis elbow) has been demonstrated to occur in up to 50% of tennis players. However, this condition is not limited to tennis players and has been reported to be the result of overuse from many activities. Lateral epicondylitis is extremely common in today's active society.
Any activity involving wrist extension or supination can be associated with overuse of the muscles originating at the lateral epicondyle. Tennis has been the activity most commonly associated with the disorder. The risk of overuse injury is increased two- to threefold in those who play more than 2 hours weekly and two- to fourfold in players older than 40 years.
Several risk factors have been identified, including improper technique, size of racquet handle, and racquet weight. For work-related lateral epicondylitis, a systematic review identified the following three risk factors((Ref5}:
The review also found that low job control and low social support were psychosocial factors associated with lateral epicondylitis.[5]
Many proposed explanations for lateral epicondylitis (tennis elbow) have involved inflammatory processes of the radial humeral bursa, synovium, periosteum, and annular ligament. However, Nirschl and Pettrone defined the basic process as microscopic tearing with formation of reparative tissue (ie, angiofibroblastic hyperplasia) in the origin of the ECRB.[6] This microtearing and repair response can lead to macroscopic tearing and structural failure of the origin of this muscle.
Concomitant intra-articular lesions (eg, loose bodies, synovitis, ulnohumeral osteophytes, chondral lesions) have been visualized during elbow arthroscopy in patients with lateral epicondylitis. However, whereas concomitant intra-articular pathology has been noted, this process is currently considered an extra-articular one.
Patients present complaining of lateral elbow and forearm pain exacerbated by use. The typical patient is a man or woman aged 35-55 years who is either a recreational athlete or one who engages in rigorous daily activities.
Upon examination, the patient has a point of maximal tenderness just distal (5-10 mm) to the lateral epicondyle in the area of the ECRB. Wrist extension or supination (but not flexion or pronation) against resistance with the elbow extended should provoke the patient's symptoms. Another helpful test is the chair raise test, in which the patient stands behind the chair and attempts to raise it by placing the hands on the top of the chair back and lifting. In patients with lateral epicondylitis, this test elicits pain over the lateral elbow.
Approximately 90-95% of patients with lateral epicondylitis (tennis elbow) respond to conservative measures and do not require surgical intervention. Patients whose condition is unresponsive to 6 months of conservative therapy (including corticosteroid injections) are candidates for surgical treatment.
The ECRB arises from the lateral epicondyle. It lies deep to the extensor carpi radialis longus (ECRL) and superficial to the joint capsule. The annular and collateral ligaments are located beneath and just distal to the origin of the ECRB.[7]
No absolute contraindications to lateral epicondylitis (tennis elbow) surgery exist. It is advisable to offer surgery only after patients have failed 3-6 months of nonoperative modalities, such as steroid injections, splinting, and occupational therapy. Relative contraindications include any comorbidities that would place the patient at a more serious level of surgical risk.
Workup
Copyright © www.orthopaedics.win Bone Health All Rights Reserved


