Calcium pyrophosphate deposition disease (CPDD) is a metabolic arthropathy caused by the deposition of calcium pyrophosphate dihydrate in and around joints, especially in articular cartilage and fibrocartilage (see the images below).[1] Although CPDD is often asymptomatic, with only radiographic changes seen (ie, chondrocalcinosis), various clinical manifestations may occur, including acute (pseudogout) and chronic arthritis. (See Etiology, Presentation, and Workup.)
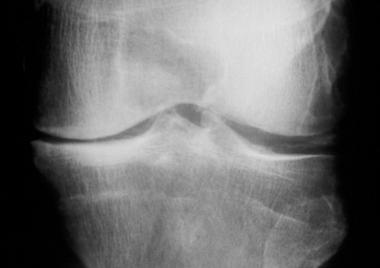 Calcium pyrophosphate deposition disease. Radiograph of the knee showing chondrocalcinosis involving the meniscal cartilage, as well as evidence of osteoarthritis.
Calcium pyrophosphate deposition disease. Radiograph of the knee showing chondrocalcinosis involving the meniscal cartilage, as well as evidence of osteoarthritis.
 Calcium pyrophosphate deposition disease. Radiograph of the wrist and hand showing chondrocalcinosis of the articular disc of the wrist and atypical osteoarthritis involving the metacarpophalangeal joints in a patient with underlying hemochromatosis.
Calcium pyrophosphate deposition disease. Radiograph of the wrist and hand showing chondrocalcinosis of the articular disc of the wrist and atypical osteoarthritis involving the metacarpophalangeal joints in a patient with underlying hemochromatosis.
Almost any joint may be involved by CPDD, although the knees, wrists, and hips are most often affected. This condition is the most common cause of secondary metabolic osteoarthritis. (See Presentation.)
According to McCarty, the five most common presentations of CPDD are as follows:
Patients with CPDD can experience significant morbidity due to the pain of an acute attack of pseudogout or to symptoms of chronic arthropathy. Treatment of symptomatic CPDD is important to prevent further end-organ damage, but it cannot reverse the joint disease.
For patient education information, see the Arthritis Center, as well as Knee Pain.
NextAlthough the exact mechanism for the development of CPDD remains unknown, increased adenosine triphosphate breakdown with resultant increased inorganic pyrophosphate in the joints results from aging, genetic factors, or both. Changes in the cartilage matrix may play an important role in promoting CPPD deposition. Rare hereditary forms of CPDD occur, generally inherited in an autosomal dominant mode.
Overactivity of enzymes that break down triphosphates, such as nucleoside triphosphate pyrophosphohydrolase, has been observed in the cartilage of patients with CPDD. Therefore, inorganic pyrophosphate can bind calcium, leading to CPPD deposition in the cartilage and synovium.[2, 3] Hyaline cartilage is affected most commonly, but fibrocartilage, such as the meniscal cartilage of the knee, can also be involved.[4]
Hypotheses based on in vitro studies propose that pyrophosphohydrolase activity and inorganic phosphate content, as noted above, are generalized phenomena that occur in fibroblasts.[5] Although these phenomena are generalized, the reason they occur only in joints remains unknown.
Genetic defects have been identified as specific gene mutations in a few kindred families.[6] The mutations were in the genes ANKH and COL, which may be involved in crystal-induced inflammation. This is related to synovial tissue and direct cartilage activation, leading to the arthritis caused by CPPD. The ANKH protein is involved in transport of inorganic pyrophosphate (PPi), which regulates calcification, bone mineralization, and bone resorption.[7]
The gene TNFRSF11B encodes osteoprotegerin, which has a critical role in regulating osteoclast development. In a study of patients with familial osteoarthritis with chondrocalcinosis, Ramos et al identified a mutation in TNFRSF11B that results in a form of osteoprotegerin with enhanced capacity to inhibit osteoclastogenesis and bone resorption.[8]
Subsequent messenger RNA expression analysis of the relevant genes in this pathway, in articular cartilage of independent patients undergoing joint replacement surgery for osteoarthritis, showed that upregulation of TNFRSF11B is a general phenomenon in the pathophysiological process of osteoarthritis.[8]
CPDD is a common condition that occurs with aging in all races. In a retrospective study of 1070 consecutive computed tomographic scans of the abdomen and pelvis in patients over 65 years of age, the prevalence of symphysis pubis chondrocalcinosis was 21.1%.[9] Nearly 50% of people older than 85 years have radiologic evidence of chondrocalcinosis.
CPDD is slightly more common in women than in men. The exact female-to-male ratio is unknown but is probably 1.4:1.
CPDD usually occurs in individuals who are in the fifth decade of life or older, with increasing prevalence as age increases. When it occurs early, before the fourth decade of life, it is usually associated with a secondary cause, such as an underlying metabolic disease, or with a familial cause.
Clinical Presentation
Copyright © www.orthopaedics.win Bone Health All Rights Reserved