In October 1989, the health department in New Mexico was notified of 3 patients with an unexplained acute illness characterized by intense myalgias and peripheral blood eosinophilia. Within weeks, a nationwide outbreak of this disease occurred. The disorder was termed eosinophilia-myalgia syndrome (EMS). In November 1989, for the purpose of nationwide surveillance, the US Centers for Disease Control and Prevention (CDC) defined this syndrome as requiring all of the following criteria: (1) incapacitating myalgias, (2) a blood eosinophil count greater than 1000 cells/µL, and (3) no evidence of infection (eg, trichinosis) or neoplastic conditions that could account for these findings.
Shortly thereafter, two case-control studies initiated by the health departments in New Mexico and Minnesota confirmed a strong association between the use of a specific brand of L-tryptophan and the development of EMS. Analyses of implicated lots of L-tryptophan identified many contaminants. The best-characterized of these is 1,1-ethylidenebis (L-tryptophan) (EBT), a tryptophan dimer. With the recall of L-tryptophan from the market in November 1989, a precipitous fall in the frequency of EMS was observed.
A new approach to constructing a criterion standard for validating diagnostic criteria for a disorder was proposed using EMS as the sample disease.[1] Case reports of patients with and without EMS were reviewed and judged by an external panel of clinical experts, thus providing independent validation of the criterion standard case reports. The proposed criteria included two EMS disease onset patterns (acute and subacute).
Contaminated L-tryptophan may not be the only cause of EMS. According to one estimate, 14% of EMS cases were not related to L-tryptophan. Non–L-tryptophan–related cases were more likely to be associated with peripheral edema, rash, sclerodermalike skin changes, alopecia, neuropathy and lower mean eosinophil count, fewer pulmonary symptoms, and a better prognosis than L-tryptophan cases. Two cases of an EMS-like illness were recently described, which closely followed the ingestion of nonprescription probiotics but not L-tryptophan. Prominent features included acute neurologic involvement with mononeuritis multiplex and necrotizing vasculitis. Features suggesting Churg-Strauss arteritis were absent, as were the edema and fibrosis characteristic of EMS.[2]
A review of toxic oil syndrome (TOS) cases that affected many thousands of Spanish patients in the early 1980s and were associated with adulterated rapeseed oil reveals that TOS shares many clinical and histopathological features with EMS. Furthermore, recent biochemical data have suggested a link between EMS and TOS. A common toxic metabolite (4-aminophenol) causes the release of dangerous carbonyl species.[3]
In an unusual experiment, an investigator injected himself subcutaneously with quinolinic acid, an L-tryptophan metabolite, resulting in peripheral blood eosinophilia and dermal and subcutaneous inflammatory lesions resembling those of eosinophilic fasciitis and increased transforming growth factor beta-1 (TGFB1) deposition.[4] Because increased serum quinolinic acid concentrations have been recorded in eosinophilic fasciitis, these data support a relationship between EMS and eosinophilic fasciitis. This finding is not surprising considering the similar clinical findings in these two disorders.
Patients with fibromyalgia syndrome (FMS) and related disorders disproportionately ingested over-the-counter L-tryptophan–containing products, but it is unknown if these individuals were predisposed to EMS. In one study, peripheral blood mononuclear cells (PBMC) from 6 of 7 patients with EMS and other functional somatic syndromes, when incubated with peak E, produced type II (profibrotic) cytokines (compared with 3 of 24 controls).[2, 5, 6, 7]
NextThe pathogenesis of EMS remains unknown. The 3 major pathological findings observed in persons with EMS include (1) capillary endothelial cell hyperplasia, with evidence of swelling and necrosis; (2) inflammatory cell infiltration, including monocytes, histiocytes, lymphocytes, macrophages, and plasma cells, and, occasionally, eosinophils in nerve, muscle, and surrounding connective tissue (eg, the subdermal fascial layer [fasciitis]); and (3) increased fibrosis, mostly in fascia but also occasionally in skin.
Levels of cytokines interleukin (IL)–2, IL-4, IL-5, interferon gamma, and granulocyte-monocyte colony stimulating factor (GMCSF) are increased in the serum of some patients with EMS. Serum soluble IL-2 receptor (sIL-2R) levels were elevated in 7 patients with EMS compared with controls. Injection of EBT in rodents caused inflammation in the dermis, fascia, and perimysium. In addition, EBT stimulates fibroblast proliferation and collagen synthesis in vitro, but eosinophilia does not develop in EBT-treated animals. The precise role of this contaminant in the pathogenesis of EMS remains uncertain.
It may be unnecessary to implicate L-tryptophan impurities in the development of EMS. Excessive oral ingestion of tryptophan supplement inhibits histamine degradation by increasing formation of formate and indolyl metabolites, several of which block the degradation of histamine, thereby potentiating its effects. Increased histamine activity is known to induce peripheral blood eosinophilia and myalgia.[8] Furthermore, patients with hypothalamic-pituitary-adrenal axis dysregulation who do not have EMS also manifest greatly increased sensitivity to ingested tryptophan and histamine. Histamine disequilibrium appears to be a final common pathway for syndromes characterized by eosinophilia with myalgia.
United States
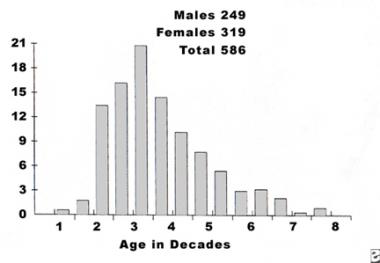
By July 1991, 1543 EMS cases in the United States had been reported to the CDC.[9] However, estimates indicate that 5,000-10,000 people actually had this disease. Since 1991, only a few new cases have been reported, most recently in 2011.[10]
International
EMS also occurred in other parts of the world, including the United Kingdom, France, Israel, Japan (12 patients), western Germany (69 patients), and Canada (10 patients). Cohort studies performed during the epidemic estimated that the attack rate of EMS among users of L-tryptophan was 0.5%-9%, depending on the product lot of the L-tryptophan ingested.
See the list below:
See the list below:
See the list below:
See the list below:
Copyright © www.orthopaedics.win Bone Health All Rights Reserved