The term Vaughan-Jackson syndrome refers to disruption of the digital extensor tendons, beginning on the ulnar side of the hand and wrist with the extensor digiti minimi (EDM) and extensor digitorum communis (EDC) tendon of the small finger. If the underlying pathology is not treated, sequential rupture of the EDC tendons of the ring, long, and index fingers occurs; ultimately, rupture of the extensor indicis proprius (EIP) may follow.[1]
OJ Vaughan-Jackson's first report of extensor tendon rupture described two elderly laborers with degenerative arthritis of the distal radioulnar joint (DRUJ).[2] He found that the tendons were frayed and disrupted directly over a bony prominence projecting from the head of the ulna in both cases. In a subsequent report,[3] he described the process of attritional rupture of the digital extensor tendons in the rheumatoid hand, with which his name has become associated. Rheumatoid arthritis (RA) is the most common underlying etiology of tendon rupture in the hand and wrist and is the usual clinical setting in which the term Vaughan-Jackson syndrome is employed.
Other, less common, patterns of tendon rupture seen in RA include rupture of the extensor pollicis longus (EPL) in the vicinity of Lister's tubercle within the third dorsal compartment[4] and rupture of the flexor pollicis longus and index-finger flexor digitorum profundus tendons within the carpal tunnel (ie, Mannerfelt syndrome).[5]
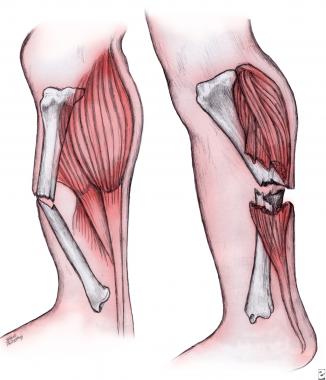
NextTendon ruptures in Vaughan-Jackson syndrome are primarily caused by gradual attrition of the tendons on the ulnar head, which, in RA, may subluxate or dislocate dorsally due to loss of the normal supporting structures. The process of tendon wear may be exacerbated by osteophytes and sharp prominences resulting from primary or secondary degenerative changes of the bone. Attrition of the tendons on the unstable distal ulnar stump after partial ulnar excision (Darrach procedure) has also been described as a cause of digital extensor tendon rupture.[6, 7]
Direct invasion of the tendons and interference with normal tendon blood supply resulting from rheumatoid tenosynovitis have also been implicated as contributing causative factors. The cascade of wrist and DRUJ deformities produced by RA often results in palmar and ulnar subluxation of the extensor carpi ulnaris (ECU) tendon, taking it out of harm's way. The ECU and stout radial wrist extensors are seldom ruptured.[4, 8, 9]
Rupture of the EPL tendon within the third dorsal compartment is occasionally seen as a complication after a minimally displaced fracture of the distal radius in patients without RA. Mechanical factors unrelated to rheumatoid disease that have been described as causes of extensor tendon rupture include the following:
Bony prominences resulting from Kienbock disease and carpal osteochondromata, as well as local inflammation related to gout and calcium pyrophosphate dihydrate crystal deposition disease (pseudogout) have also resulted in tendon rupture.[10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20]
Risk factors that have been associated with digital extensor tendon rupture in RA patients include the following:
 Posteroanterior radiograph of the wrist following wrist arthrodesis and resection of the distal ulna displays the scallop sign, which is the term used to describe the scooped-out appearance of the sigmoid notch of the radius that results from synovial proliferation and bone erosion.
Posteroanterior radiograph of the wrist following wrist arthrodesis and resection of the distal ulna displays the scallop sign, which is the term used to describe the scooped-out appearance of the sigmoid notch of the radius that results from synovial proliferation and bone erosion.
In a study of 58 rheumatoid hands with tendon rupture,[22] 73% of the hands had two or more of these risk factors, and 93% of the patients with tendon rupture were noted to have persistent tenosynovitis for 6 months, making this finding particularly worrisome.
A review of 41 wrists with extensor tendon rupture due to DRUJ osteoarthritis found that tendon disruption occurred only in those joints with severe radiographic changes.[23] Specifically, widening and deepening of the sigmoid notch of the radius (the scallop sign) was the radiographic finding most strongly associated with tendon rupture in these osteoarthritic patients.
In the United States, the vast majority of tendon ruptures occur in patients with RA, and the incidence of extensor tendon involvement is 10-15 times that of involvement of the flexor tendons. Although some studies have reported tendon rupture to be more common in the dominant hand, this has not been a universal finding.[4]
Tendon rupture caused by osteoarthritis, though relatively rare, is more common in older persons, whereas no age restriction exists for tendon rupture caused by RA. The pattern of rheumatoid joint involvement can vary dramatically among individuals, sometimes even from one extremity to the other in the same patient. Tendon ruptures have been seen in patients who have had RA for as little as 2 years to as long as 25 years, though in most series, rheumatoid disease has been present for an average of 10-15 years.[24]
Hands with single-digit tendon ruptures exhibit better results than do those with multiple-digit involvement.[4, 25] In particular, extension lag following reconstruction seems to increase in direct proportion to the number of digits involved.[26] A functional 70° arc of MCP joint motion is commonly restored.[4] Delays in initiating surgical treatment are sometimes associated with poorer outcomes, although this is not a universal finding.[25, 26]
Patients with RA are remarkably adept at coping with hand deformity and dysfunction. In patients with relatively normal MCP joint function, loss of the ability to extend the digits and open the hand to grasp large objects imparts obvious functional limitations. Other individuals with severe MCP joint deformity or subluxation may not even be aware that extensor tendon rupture has occurred.
The services of a certified hand therapist are invaluable in educating patients on the postoperative regimen. Splint use and activity restriction must be adhered to in order to prevent disruption of the tendon graft or transfer.
Perhaps the most important lesson that can be imparted to these patients is an understanding of the warning signs and risk factors that may indicate the possibility of impending tendon rupture in the contralateral limb.
Clinical Presentation
Copyright © www.orthopaedics.win Bone Health All Rights Reserved