A basic knowledge of the signs and symptoms of acute spinal cord dysfunction are required in order to perform a relevant history and physical examination. A spinal sensory level is classically found, but sensory complaints and findings limited to the distal extremities can also be seen early in the course of spinal infarction. Typically onset is apoplectic, evolving in minutes or a few hours to produce severe dysfuction of sensory and motor systems.
NextOcclusive vascular lesions affecting the spinal cord (spinal stroke) are diagnostic challenges. As is the case for the more common cerebrovascular accident affecting cerebral circulation, an acute onset is a clue to the diagnosis. The circulation to the spinal cord has unique features related to the rich anastomotic anatomy of the cord that result in relative rarity of spinal cord infarction in comparison to cerebral infarction, as described in the images below.
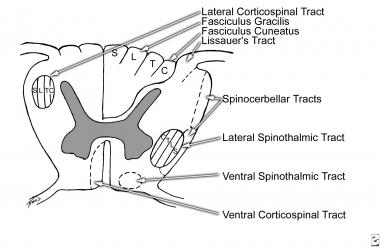 Transverse section of spinal cord showing location of main pathways. The lamination of fibers in posterior columns and in lateral spinothalamic and lateral corticospinal tracts is indicated (C, cervical; T, thoracic; L, lumbar; S, sacral).
Transverse section of spinal cord showing location of main pathways. The lamination of fibers in posterior columns and in lateral spinothalamic and lateral corticospinal tracts is indicated (C, cervical; T, thoracic; L, lumbar; S, sacral).
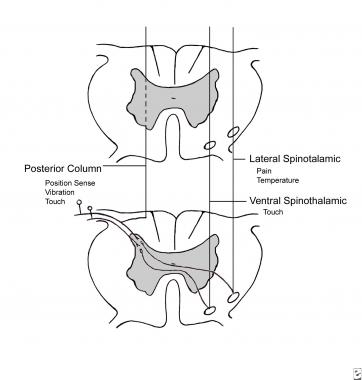 Simplified representation of course of major sensory pathways in the spinal cord. Decussation of the spinothalamic tracts occurs within one or two segments of their entry.
Simplified representation of course of major sensory pathways in the spinal cord. Decussation of the spinothalamic tracts occurs within one or two segments of their entry.
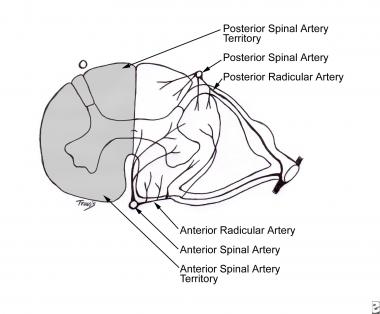 Pattern of arterial supply to spinal cord and (left) territories of the anterior and posterior spinal arteries.
Pattern of arterial supply to spinal cord and (left) territories of the anterior and posterior spinal arteries.
The anterior spinal artery is a single long anastomotic channel that lies at the mouth of the anterior central sulcus and supplies the circulation to the anterior two thirds of the spinal cord, shown below.
Pattern of arterial supply to spinal cord and (left) territories of the anterior and posterior spinal arteries.
It gives origin to sulcal arteries that take an arching course to one or the other anterior gray horns. The posterior spinal arteries are smaller paired arteries lying just medial to the dorsal roots. The arterial supply of the spinal cord arises from the aorta and at its cephalad and caudal ends from tributaries of the subclavian and iliac arteries. Eight to ten unpaired anterior medullary arteries are branches of the larger afferent aorta and vertebral and iliac arteries. The largest anterior medullary artery, the great anterior medullary artery of Adamkiewicz, which is susceptible to occlusion with neurologic deficit, is located at the lumbar enlargement, usually at L2 on the left side (but may be at any point from T8 to L2).
United States
Spinal cord infarction is not common, but only fragmentary or indirect data are available on incidence or prevalence. A large study showed that only 9 of 3784 autopsies revealed spinal cord infarction, with a rate of occurrence of 0.23% at death. Conversely, if spinal stroke is approximately 1.2% of strokes, an overall annual incidence of 12 in 100,000 can be estimated.
International
International incidences are also unclear. Recent reports that describe patients developing spinal cord infarction in an increasing number of situations and pathologies would influence this because procedures ranging from major surgery to injections for epidural anesthesia, infections and especially meningitis, and medications vary in different countries.
The risk to life and its quality from spinal cord infarction is substantial because of the disability, which can be severe, with paraplegia, risk of pulmonary emboli, and risk of infection (eg, bladder, lungs, decubiti). However, no epidemiologic studies are available because of the relatively small number of patients affected.
Published series of reports of spinal cord infarction are relatively small, ranging up to 36-44 patients.[1] They find a mortality rate in the vicinity of 20-25% for patients admitted to hospital with spinal cord infarction.[2] No relationship to age is reported. However, the reported series do have a median age of 52 years.
Although prognosis is guarded, with many or most patients remaining severely weak and with with severe bladder dysfunction, up to one-third to one-half of patients experience slow recovery of at least a moderate nature.
Clinical Presentation
Copyright © www.orthopaedics.win Bone Health All Rights Reserved