A freely moveable synovial joint links the upper extremity to the torso, with the sternoclavicular joint (SCJ) participating in all movements of the upper extremity. The SCJ is a saddle-type joint that provides free movement of the clavicle in nearly all planes. The ability to thrust the arm and shoulder forward requires sound function of the SCJ. Because only about 50% of the medial end of the clavicle articulates with the manubrium, the SCJ has little inherent stability. Most of the SCJ's strength and stability originates from the joint capsule and supporting ligaments. The capsule surrounding the joint is weakest inferiorly, while it is reinforced on the superior, anterior, and posterior aspects by the various ligaments, including the interclavicular, anterior and posterior sternoclavicular, and costoclavicular ligaments.
In a cadaver study of the structures of the sternoclavicular joint, 11 joints from 4 men and 7 women were dissected to identify relevant surgical landmarks. The clavicular pectoralis ridge served as a reliable osseous landmark for reference to the soft-tissue attachments around the sternoclavicular joint. The costoclavicular ligament was the largest ligament of the sternoclavicular joint, with 80% greater footprint area than that of the posterior sternoclavicular ligament. Articular cartilage covered 67% of the medial end of the clavicle and was located anteroinferiorly. An avascular plane that can serve as a "safe zone" for posterior dissection was observed in each specimen, posterior to the sternoclavicular joint and anterior to the sternohyoid and sternothyroid muscles.[1]
NextUsually only through the application of significant force do the ligaments supporting the SCJ become completely disrupted, enabling dislocation of the joint. Whether the SCJ subluxes or dislocates depends on the extent of the damage to the supporting ligaments and capsule. Sternoclavicular joint injuries (SJIs) are graded into 3 types.
A significant direct or indirect force to the shoulder region can cause a traumatic dislocation of the SCJ.[2] Anterior dislocations of the SCJ are much more common (by a 20:1 ratio), usually resulting from an indirect mechanism such as a blow to the anterior shoulder that rotates the shoulder backward and transmits the stress to the joint[3] . Traumatic contact driving the shoulder forward can cause posterior dislocations of the SCJ, as can direct impact to the superior sternal or medial clavicular surfaces.
United States
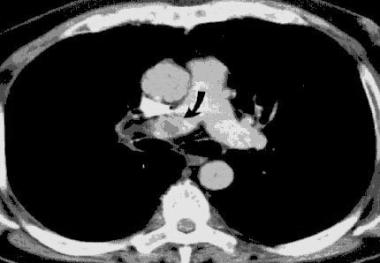
The ligaments and capsule of the SCJ contribute enough stability to make this one of the least dislocated joints in the body. Sternoclavicular dislocations are uncommon, accounting for only 3% of a series of 1603 shoulder girdle injuries. Posterior dislocations are considerably less common than anterior dislocations. Only 1 patient in the cited series of 1603 shoulder girdle injuries had a posterior dislocation. However, the proportion of reported mediastinal complications seems to have risen. This may be due to either reporting bias or due to detection bias with the increased use of CT scanning and its increased sensitivity.
Mortality and significant morbidity occur infrequently with anterior dislocations of the SCJ.[4, 5, 6, 7] Problems are usually related to issues of physical appearance as well as pain and functional limitations for persons with an active lifestyle.
However, a posterior SCJ dislocation has the potential for severe and even life-threatening complications. Case reports of such complications have included the following:
These and other complications can cause significant disability, including even cerebrovascular accident and death.[4, 8, 5]
Overall incidence of sternoclavicular joint injury is higher in males than in females, probably because of the activities (eg, motor vehicle crash, contact sports) associated with the injury. However, recurrent atraumatic anterior subluxation of the SCJ (usually associated with overall joint laxity) though rare, occurs more frequently in young girls.
Incidence is increased in young adult males, since this population is engaged more often in activities associated with SJI, such as motor vehicle crashes and contact sports.
In patients younger than age 25, a true sternoclavicular separation may not occur. A physeal disruption causing clavicular displacement may present with similar signs and symptoms[9] .
Clinical Presentation
Copyright © www.orthopaedics.win Bone Health All Rights Reserved