Marfan syndrome (MFS) is a spectrum of disorders caused by a heritable genetic defect of connective tissue that has an autosomal dominant mode of transmission.[1, 2, 3, 4] The defect itself has been isolated to the FBN1 gene on chromosome 15, which codes for the connective tissue protein fibrillin.[1, 5, 6] Abnormalities in this protein cause a myriad of distinct clinical problems, of which the musculoskeletal, cardiac, and ocular system problems predominate.[2, 7, 8]
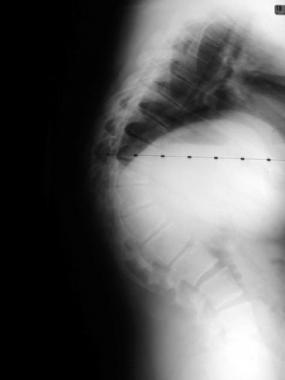
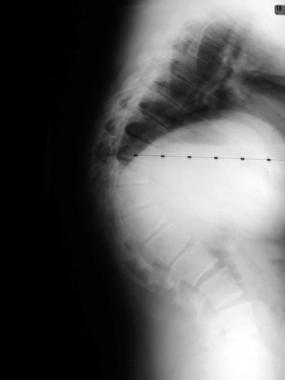
The most severe of these clinical problems include aortic root dilatation and dissection, which have historically been the causative factors in early patient demise.[9] Skeletal deformities such as thoracolumbar scoliosis, thoracic lordosis, and pectus excavatum, may lead to pulmonary difficulties that include restrictive airway disease and cor pulmonale if the deformities are progressive and untreated. Finally, blindness may result from unrecognized and untreated glaucoma, retinal detachment, and cataracts.
The skeleton of patients with MFS typically displays multiple deformities including arachnodactyly (ie, abnormally long and thin digits), dolichostenomelia (ie, long limbs relative to trunk length), pectus deformities (ie, pectus excavatum and pectus carinatum), and thoracolumbar scoliosis.[10, 11]
In the cardiovascular system, aortic dilatation, aortic regurgitation, and aneurysms[12] are the most worrisome clinical findings.[1, 3, 4] Mitral valve prolapse that requires valve replacement can occur as well. Ocular findings include myopia, cataracts, retinal detachment, and superior dislocation of the lens.[13]
Antonin Bernard Jean Marfan, whose name this syndrome bears, was born in Castelnaudary, Aude, France on June 23, 1858. In 1892, he was appointed assistant professor of pediatrics in the Paris faculty. Marfan described the disease that still bears his name at a meeting of the Medical Society of Paris in 1896. He presented the case of a 5-year-old girl named Gabrielle, who had disproportionately long limbs.
In later studies, further anomalies were documented, including arachnodactyly (long digits), cardiovascular abnormalities, and dislocation of the ocular lens. A common and often lethal complication of MFS is dissection of the aorta, and the genetic inheritance is now known to be autosomal. Marfan gained an international reputation and was widely recognized as a pioneer of pediatric medicine in France. This was very much the case in Britain, too, where he received an honorary fellowship of the Royal Society of Medicine in 1934.
NextOver many years, several investigators have studied various molecules found in the extracellular matrix in attempts to elucidate the cause of MFS.[14, 15] These molecules have included collagen, elastin, hyaluronic acid, and, more recently, fibrillin. Sakai et al identified fibrillin, a 350-kd protein, by using monoclonal antibodies raised against myofibrils.[16] Immunofluorescence studies were then used to compare the reactivity in both healthy subjects and those with MFS. During this period, similar technology was used to construct a genetic exclusion map that led to the localization of the defect to chromosome 15 (bands q15-q23).
Several point mutations have now been identified in the fibrillin gene, most of which affect cysteine residues within the microfibril. Thus, these mutations are thought to cause defective fibrillin to be produced. Fibrillin's structure and function are altered by abnormal protein folding due to the alteration of bonding between cysteine residues, which in turn causes defective microfibril production.
Mutations in the FBN1 locus of the fibrillin gene on chromosome 15 have been linked to MFS and other distinct clinical entities with similar findings.
The estimated incidence of MFS ranges from 1 in 5000 to 2-3 in 10,000 persons.[1] The mutation in the fibrillin gene causes pleiotropic effects; thus, a wide range of phenotypic features is derived from a single gene mutation. Several other diseases have presentations similar to MFS, making it exceedingly difficult to determine the exact incidence.
Advances in the management of the cardiovascular manifestations of MFS have led to a significant decrease in the morbidity and mortality that are associated with this condition. Before the advent of pharmacologic and surgical therapy for aortic root and valvular disease, the life expectancy for patients with MFS was about two thirds that of the healthy population. Aortic dissection and congestive heart failure due to aortic and mitral valvular anomalies accounted for over 90% of the known causes of death.
Patient longevity now approaches that of persons without MFS, although cardiovascular compromise is still the most common cause of patient death, likely due to sudden death in the previously undiagnosed patient and a new diagnosis in those whose disease process has progressed beyond the scope of medical or surgical cure.
Clinical Presentation
Copyright © www.orthopaedics.win Bone Health All Rights Reserved