Kyphosis refers to the normal apical-dorsal sagittal contour of the thoracic and sacral spine. As a pathologic entity, kyphosis is an accentuation of this normal curvature. Kyphosis can occur as a deformity solely in the sagittal plane, or it can occur in association with an abnormality in the coronal plane, resulting in kyphoscoliosis. Many potential etiologies of kyphosis have been identified.
An image depicting Scheurmann kyphosis can be seen below.
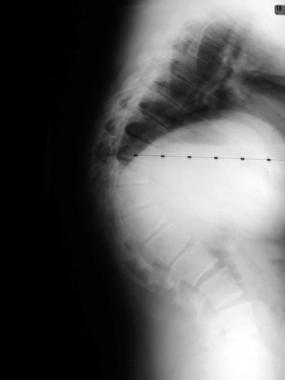 Preoperative lateral of a patient with an 85° thoracic deformity secondary to Scheuermann kyphosis.
Next
Preoperative lateral of a patient with an 85° thoracic deformity secondary to Scheuermann kyphosis.
Next
Normal kyphosis is defined as a Cobb angle of 20-40° measured from T2-T12.[1, 2]
Pathologic kyphosis can affect the cervical and lumbar spine as well the thoracic spine, but cervical and lumbar involvement is uncommon. Any kyphosis in these areas is abnormal.
Kyphosis can cause pain and potentially lead to neurologic deficit and abnormal cardiopulmonary function.
Many potential causes of kyphosis have been described.[3] Scheuermann disease and postural round back are often identified in adolescents.[4, 5, 6] Congenital abnormalities, such as failure of formation or failure of segmentation of the spinal elements, can cause a pathologic kyphosis. Autoimmune arthropathy, such as ankylosing spondylitis, can cause rigid kyphosis to develop as the spinal elements coalesce. Kyphosis can also develop as a result of trauma, a spinal tumor, or an infection. Iatrogenic causes of kyphosis include the effects of laminectomy and irradiation, which lead to incompetence of the anterior or posterior column. Finally, metabolic disorders and dwarfing conditions can lead to kyphosis.
This article focuses on kyphosis due to Scheuermann disease and postural, postinfectious, posttraumatic, or iatrogenic etiologies.
The pathophysiology of kyphosis depends on the etiologic factor. The exact cause of Scheuermann disease is still imprecisely defined. Scheuermann postulated that the condition resulted from avascular necrosis of the apophyseal ring. Other theories include histologic abnormalities at the endplate, osteoporosis,[7] and mechanical factors that affect spinal growth.[8] A Danish study demonstrated an important genetic component to the entity.[9]
Postural kyphosis is present when accentuated kyphosis is observed without the characteristic 5° of wedging over 3 consecutive vertebral segments that defines Scheuermann kyphosis.[10] This is felt to be due to muscular imbalance leading to the round-back appearance of these individuals.
When focal kyphosis occurs after a fracture, more height is lost in the anterior aspect than in the posterior aspect; this is the typical fracture pattern. The angulation can increase as the fracture heals, placing pressure on the spinal cord. Patients with fractures have historically been treated with laminectomy alone, especially in the thoracic spine, and they often had progressive kyphosis at the fracture site.[11, 12]
Postinfectious kyphosis occurs in a manner similar to that just described. Mechanical integrity of the anterior column is lost due to the infectious process. Bending forces then accentuate the normal sagittal contour.
Patients with a symptomatic kyphosis often present with axial back pain. They may also be concerned about the cosmesis of their rounded back.
Patients with kyphosis should be carefully questioned about and examined for neurologic problems, especially myelopathy. Difficulty with gait and hyperreflexia should prompt further investigation of the kyphosis.
A 10- to 42-year, natural-history study of Scheuermann disease revealed that patients, as compared with a control group, tended to have increased back pain.[13] However, they were not more likely than the control group to take pain medication, to have sedentary jobs, or to lose motion of the spine. The investigators found no differences in educational level, absenteeism, self-consciousness, or reports of numbness in the legs. Of interest, restrictive lung disease was observed in patients with a curve greater than 100°.
Indications for treatment of kyphosis include unremitting pain, neurologic changes, progression of deformity,[14] and cosmesis.[8] Indications for surgical treatment of Scheuermann kyphosis have changed fairly substantially; however, precise indicators have not been elucidated.
Authors from early clinical series simply cited pain or deformity as reasons to perform fusion. Proposed indications more specific than these are kyphosis greater than 75°, kyphosis greater than 65° with pain, and an unacceptable appearance of the trunk.[15]
Other possible indications in severely affected patients are problems with balance while sitting and skin problems due to pressure at the apex of the deformity.
Surgical intervention for posttraumatic kyphosis is recommended if the patient's neurologic status changes, if the condition progresses, if the kyphosis is 30° or more, or if the loss of anterior vertebral height is more than 50%.[16]
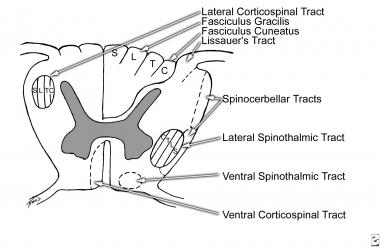
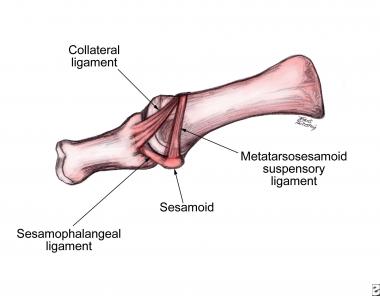
Detailed working knowledge of the anatomy of the spine is essential for the treatment of kyphosis.
Contraindications to surgery for kyphosis include a clinically significant cardiopulmonary risk and medical unfitness for surgery.
Workup
Copyright © www.orthopaedics.win Bone Health All Rights Reserved