When a bursa becomes inflamed, it may be categorized as either septic (infective) or aseptic (noninfective). Aseptic bursitis is a sterile inflammation, which may occur secondary to acute trauma, overuse injury, crystal deposition (eg, gout, pseudogout), or systemic disease (eg, rheumatoid arthritis [RA], uremia, systemic lupus erythematosus). Aseptic cases account for approximately two thirds of all bursitis diagnoses.
Septic bursitis is the inflammation of a bursa secondary to the seeding of the bursal sac with microorganisms; most commonly, these microorganisms are bacteria, but they can, rarely, be fungus or algae. Seeding most often occurs transcutaneously after trauma to the region overlying the bursa.[1, 2]
Clinically, septic bursitis is difficult to distinguish from its aseptic counterpart. Roughly 40% of patents with septic bursitis are found to have clinically significant fever (>38°C/100.4°F). Bursal warmth is almost uniformly noted in infective cases but is observed only 50% of the time in those with no infection. Peribursal cellulitis is noted in more than 60% of septic bursitis cases but only 25% of noninfective cases.
It should be recognized, however, that a clear diagnosis of cellulitis can be difficult, in that the findings of erythema, increased warmth, and tenderness may be local inflammatory changes rather than true peribursal cellulitis. Tenderness is usually present in all bursitis cases; however, the degree of tenderness seems to be far more pronounced in septic bursitis than in aseptic bursitis.[3]
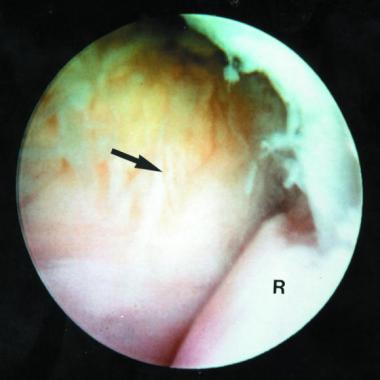
NextAspiration of of an inflamed olecranon bursa is performed to obtain fluid for analysis. Noninfective (aseptic) bursitis is distinguished from infective (septic) bursitis.
Definitive diagnosis of septic bursitis can be made only by culture isolation of the causative organism. Bursal aspirates in septic cases almost always have markedly elevated white blood cell (WBC) counts (>100,000/µL) with a predominance of neutrophils. Fluid from an inflamed aseptic bursa may show a moderately increased WBC count; however, the predominant cell type is mononuclear. In addition, a bursal fluid glucose–to–serum glucose ratio lower than 50% is virtually exclusive to septic bursae.[4, 5]
Whereas olecranon bursitis is usually sterile, the olecranon bursa is the most frequent site of septic bursitis and, therefore, should not be injected with steroids before fluid analysis.[6]
Contraindications for aspiration of the olecranon bursa include the following:
Copyright © www.orthopaedics.win Bone Health All Rights Reserved