Intractable plantar keratosis (IPK) is a focused, painful lesion that commonly takes the form of a discrete, focused callus, usually about 1 cm, on the plantar aspect of the forefoot. Typically, IPKs occur beneath one or more lateral metatarsal heads or under another area of pressure.[1, 2, 3, 4] Although the diagnosis of IPK is made clinically, the differential diagnosis includes plantar verrucous carcinoma[5] and epidermal inclusion cyst.[6] The pain associated with IPK can limit ambulation and also cause compensatory changes in gait.
IPK is often treated successfully with nonoperative care. Those lesions that continue to cause pain may require surgical intervention. Various surgical procedures have been described for treatment of IPK, ranging from partial metatarsal excisions to metatarsal osteotomies and shortening procedures or, in the case of the first ray, sesamoid surgery.
Henri DuVries reported on metacondylectomy in 1953. This technique involves removal of a portion of articular surface of the metatarsal and the plantar condyle. The procedure completely resolved the lesion in 79% of patients and was associated with a 93% patient satisfaction rate.[7]
Hatcher et al presented a thorough review of 238 various metatarsal osteotomies used in the correction of IPK. The overall success rate was only 56.5%; this was thought to be due to the fact that transfer lesions occurred in almost 40% of the patients.[8]
Several different distal osteotomies are described, including the dorsal V (or chevron) osteotomy, the tilt-up wedge osteotomy, and the free-floating osteoclasis technique.
The chevron osteotomy of the distal metatarsal, with dorsal displacement of the metatarsal head, is frequently reported. Dreeben et al found complete relief of symptoms in 67% of 45 patients in whom this method was used.[9] Young and Hugar likewise used the chevron osteotomy, and they achieved an 87.5% success rate in resolving symptomatic IPK.[10]
A later modification of the DuVries technique is to remove just the plantar condyle, through a dorsal approach. This significantly reduces the chance of transfer lesions, because no change is made to the weightbearing metatarsal parabola.
An isolated IPK beneath the first metatarsal is often caused by a hypertrophic sesamoid bone. Historically, this was treated with tibial or fibular sesamoidectomy. Sesamoid shaving or planing has met with good success and fewer complications.[11]
For patient education materials, see the Foot, Ankle, Knee, and Hip Center.
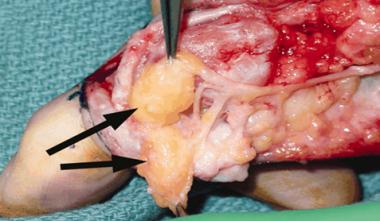
NextA plantar or dorsally displaced metatarsal alters the pressure pattern in the forefoot, and an IPK can form in the area of increased pressure. Typically, this is beneath one of the lesser metatarsal heads and can be exacerbated by a hammertoe deformity or hypertrophic metatarsal condyles. These condyles are small protuberances on the plantar flare of the metatarsal head that serve as a soft-tissue attachment point. In some cases, these condyles become enlarged and cause focused pressure beneath the metatarsal head.[12]
IPKs beneath the great toe are somewhat different. Beneath the first metatarsophalangeal (MTP) joint are two small bones called sesamoids, which are embedded within the soft tissues. The toe flexors pass underneath the first MTP joint, and the sesamoids act as a fulcrum, similar to the patella in the knee. The sesamoids also help to absorb pressure under the foot during standing and walking, and they ease friction in the soft tissues under the toe joint when the big toe moves. Malalignment of or a fracture in the sesamoids can contribute to the development of IPK.
The metatarsal parabola, or cascade, should be assessed when surgical intervention is under consideration. In the typical cascade, the second digit is longer than (or sometimes as long as) the first, followed in length by, from longest to shortest, the third, fourth, and fifth digits. This permits the natural transition of weightbearing forces across the forefoot. If this cascade is altered, either in metatarsal length or in the metatarsal head position in the sagittal plane, this can create an IPK.
The pathophysiology of IPK involves an impairment of normal weightbearing and a resultant increase in the thickness of the stratum corneum of the sole of the foot. As the lesion develops, the central portion invaginates and becomes extremely painful.
A focused area of pressure on the plantar fat pad, typically resulting from a dropped—or, more correctly, plantarflexed—metatarsal, causes IPK. In such cases, the metatarsal head lies in a plane lower than the surrounding metatarsals, focusing exaggerated weightbearing stress on this area.
Other causes of IPK include tight or poorly fitting shoes, hammertoe deformity, long lesser metatarsals, hypertrophic plantar metatarsal head condyles, malunion of metatarsal fracture, accessory sesamoids, and first-ray hypermobility.
In poorly fitting shoes, the toes may become buckled in a tight toe box and create a retrograde hammertoe effect. This forces the toe on top of the lesser metatarsal head and drives the head down against the plantar fat pad. Long lesser metatarsals also have added weightbearing stress shifted to them, and this shift can cause an IPK. A hypermobile first ray shifts weightbearing stress laterally and potentially overloads the plantar fat pad.
An IPK beneath the first metatarsal head is often caused by hypertrophy of either the fibular or tibial sesamoid. Other possible causes include a plantarflexed first ray, a hammered great toe, a cavus foot deformity, or excessive pronation.
Plantar keratosis can be linked to obesity and diabetes; the association was found in about 10% of patients studied in a series of 109 patients in Spain.[13]
IPK is not uncommon, but its exact frequency remains to be defined.
A successful outcome is based on accurately identifying the etiology of the IPK and clearly establishing realistic expectations. If the underlying cause is not addressed, the outcome will be poor and the patient unhappy.
Conservative, nonoperative treatments should not be discounted: Often, they are all that is required for patient relief. A study by Kang et al found that the use of metatarsal offloading pads reduced peak pressures and improved subjective pain responses in patients.[14]
Mann and Wapner reported on tibial sesamoid shaving in 10 patients with symptomatic IPK below the first metatarsal. At an average follow-up of 52.6 months, nine of the 10 patients reported good to excellent results, and one described results as fair.[11]
For the more typical lesser-metatarsal IPK, one of the various metatarsal procedures may be used. The difficulty with the majority of the metatarsal osteotomies is the unpredictable degree of dorsal displacement. Intraoperatively, it is difficult to accurately gauge the level of the metatarsal heads in the sagittal plane. The use of internal fixation reduces the chance that weightbearing will cause unwanted dorsal displacement.
Kiviniemi et al treated 25 plantar callosities in 13 patients (mean age, 48 years; five male, eight female) with transverse distal metatarsal osteotomy. Osteotomies united primarily in 24 cases and in one after revision. Twenty-three of the callosities healed, two of them after an oblique repeat osteotomy; follow-up extended 7 years. In four of the treated feet, eight hammertoe deformities developed in the involved rays. In five of the feet, eight plantar callosities developed outside the operated rays.[15]
The distal chevron is reported in multiple studies. Kitaoka and Patzer reviewed 21 feet that had undergone chevron osteotomy on the lesser metatarsals; the mean follow-up period was 4 years. Sixteen feet were labeled as good, two as fair, and three as poor. Transfer metatarsalgia occurred in three feet (14%).[16]
Idusuyi et al found that although the single oblique lesser-metatarsal osteotomy may be successful, 50% of the patients studied continued to have some degree of pain, and most patients had limitations in footwear.[17]
A study by Grimes and Coughlin on the Weil osteotomy concluded that a proximal shift of the distal osteotomy may also shift in a plantar direction. They recommended that if a shift of more than 5 mm is needed, a 2-mm-thick blade be used to allow for some dorsal displacement, in order to prevent plantar pressures.[18]
Another study on the clinical results of the Weil osteotomy found relief of plantar pain in 97% of patients treated, at a follow-up of 26 months.[19]
Proximal metatarsal segmental resection involves resection of a cylindrical segment of proximal metatarsal bone approximately 0.5 cm long. Spence et al reported good results in 54 patients operated on with this procedure.[20]
Overall, surgical intervention for lesser-metatarsal IPK should be undertaken with caution. Pontious et al reviewed 29 patients who altogether had undergone 40 V-shaped osteotomies for IPK. The overall effectiveness was quite limited, and there were multiple complications. More than 42% of the patients developed transfer lesions, 10% had recurrence, and 25% reported lack of toe purchase.[21]
Clinical Presentation
Copyright © www.orthopaedics.win Bone Health All Rights Reserved