Patients complaining of back pain after motor vehicle accidents or falls from significant heights should be considered to have spinal injuries until proven otherwise. With flexion-distraction mechanisms such as those observed in passengers restrained with lap seatbelts, a progression of injury from the posterior column of the thoracolumbar spine is observed anteriorly.[1] When this involves only the osseous structures, a Chance injury exists.
First described in 1948, the Chance fracture represents a pure bony injury extending from posterior to anterior through the spinous process, pedicles, and vertebral body, respectively.[2] The Chance fracture most commonly is found in the upper lumbar spine, but it may be observed in the midlumbar region in children. The fracture occurs at a lower level in children because of their lower center of gravity.[3]
The diagnosis is best made on good quality radiographs obtained in two planes (anteroposterior [AP] and lateral). Prompt recognition followed by appropriate reduction and immobilization usually results in a good clinical outcome. Associated intra-abdominal injuries are common,[4, 5, 6] especially in the pediatric age group,[7, 8] in which incidence approaches 50%. Thus, intra-abdominal trauma should always be excluded at the time of presentation.
NextSurgery generally has not been used to treat this injury. Because Chance fracture is a pure bony lesion and reduction is readily obtainable with extension, closed management of this injury has been the treatment of choice.
Flexion-distraction forces are responsible for the Chance fracture, which is one of the three injuries resulting from this mechanism. Usually related to lap seatbelt use, this mechanism can result in complete ligamentous injury or a combination of bony, ligament, and disc involvement.[1, 3, 9]
If a Chance fracture goes unrecognized, it may result in progressive kyphosis with ensuing pain and deformity.[10] Associated intra-abdominal injuries can result in increased morbidity and mortality.
Fewer than 10% of fractures involving the lumbar spine are a result of flexion-distraction forces. These injuries tend to occur between T12 and L4, with the highest incidence at L2.
The most common history is that of a back-seat passenger who was involved in a motor vehicle accident while restrained by a lap seatbelt[3] or that of a person who fell from a height.
Hu and Lieberman reported a case in which a 67-year-old woman with osteoporosis and thoracic kyphosis experienced a proximal vertebral body Chance fracture after pedicle screw instrumentation and fusion.[11]
The thoracolumbar spinal junction represents a transitional area from the rigid thoracic spine to the more mobile lumbar region. The thoracic spine's intrinsic stability is a result of the ribs and their articulation with the spine, the smaller disc spaces, and the frontal orientation of its facet joints. As the lower two thoracic vertebrae (T11-12) lose the anterior rib articulations (floating ribs), the facet joints also change orientation to become more oblique or sagittal, allowing an increase in mobility.[12]
Flexion-distraction forces are responsible for the Chance fracture. Usually related to lap seatbelt wear, this mechanism can result in complete ligamentous injury or a combination of bony, ligament, and disc involvement. (See the image below.)
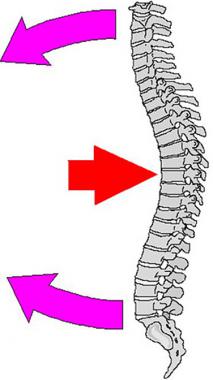 Chance fracture or modified compression fracture of upper lumbar spine may occur when weight of upper body moves forward (red arrow) while person's waist and upper body are fixed in position by seatbelt or steering wheel of automobile (pink arrows). Consequent fixed-position stress results in fracture.
Chance fracture or modified compression fracture of upper lumbar spine may occur when weight of upper body moves forward (red arrow) while person's waist and upper body are fixed in position by seatbelt or steering wheel of automobile (pink arrows). Consequent fixed-position stress results in fracture.
The patient has back pain and, on clinical examination, may have a lap seatbelt abrasion across the abdomen. It is vital to be mindful of the high incidence of associated intra-abdominal injuries, such as liver or spleen lacerations, bowel rupture, or pancreatic injury. Therefore, a thorough examination of the abdomen at the initial evaluation is of utmost importance.
It is wise to ask for a general surgical consultation at this time to ensure that an occult bowel or other viscus injury is not overlooked. Although neurologic findings are uncommon with this injury, it is nonetheless important to perform a thorough neurologic examination that includes motor, sensory, and reflex evaluation. A rectal and bladder examination should also be performed, including evaluation of the residual urine after the patient has voided. Palpation of the thoracolumbar spine is performed to assess points of maximum tenderness and palpable defects.
Radiographic assessment should begin with AP and lateral radiographs of the thoracolumbar spine. A demonstrable fracture line may be detected extending through the spinous process, pedicles, and vertebral body. In general, the diagnosis may be determined on the basis of plain radiographs, but occasionally, computed tomography (CT) scans with frontal and sagittal reconstructions are beneficial.
Although Chance fractures may generally be managed by means of closed reduction and immobilization in a thoracolumbosacral orthosis (TLSO) or hyperextension cast, surgery may be indicated for polytrauma patients or patients whose size makes closed treatment difficult or impractical.
The usual location for Chance fractures is at the thoracolumbar junction (T10-L2) in adults or the midlumbar spine in the pediatric age group. The fracture lines are found to propagate from the spinous process posteriorly through the lamina, pedicles, and vertebral body anteriorly.
Conceptually, the thoracolumbar spine may be visualized as comprising three columns, as described by Denis.[13] The anterior column is represented by the anterior half of the vertebral body, disc, and anterior longitudinal ligament. The middle column consists of the posterior half of the vertebral body, its associated disc, and posterior longitudinal ligament. The posterior column includes the pedicles, facet joints, lamina, and spinous and transverse processes, as well as the ligamentous complex, including the ligamentum flavum.
The anterior and middle columns both are primarily involved in resisting axial loading of the spine. The added importance of the middle column relates to its proximity to the spinal canal and neural elements. Displacement of the middle column can result in neurologic compression and deficits. The posterior column primarily resists tensile forces, such as those encountered in flexion-distraction injuries. In Chance fractures, the bony elements involved fail, with the ligamentous components remaining intact. (See the image below.)
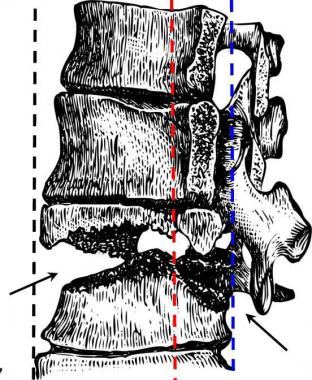 Drawing of Chance fracture of thoracolumbar junction. Defect follows irregular horizontal plane (arrows), which results in disruption of anterior (black dotted line), middle (red dotted line), and posterior columns (blue dotted line).
Drawing of Chance fracture of thoracolumbar junction. Defect follows irregular horizontal plane (arrows), which results in disruption of anterior (black dotted line), middle (red dotted line), and posterior columns (blue dotted line).
Exogenous obesity may be a relative contraindication to the usual nonoperative management of Chance fractures because it may render bracing difficult. In these instances, and in cases of multiple trauma, an operative approach may be indicated to stabilize these injuries.
Workup
Copyright © www.orthopaedics.win Bone Health All Rights Reserved