Cartilage tumors vary in severity from benign enchondroma to low-grade malignant chondrosarcoma to the highest-grade dedifferentiated chondrosarcoma. Chondrosarcoma is the second most common primary malignant bone tumor, accounting for 10-20% of all primary bony malignancies.[1, 2] Enchondroma, which consists of benign endosteal cartilage, is much more common than chondrosarcoma. The true incidence of cartilage tumors is unknown because many are discovered incidentally.
Distinguishing benign cartilage tumors from low-grade malignant cartilage tumors is often challenging, but there are some established principles regarding location, size, and pain, as well as characteristics on radiography, computed tomography (CT), and magnetic resonance imaging (MRI), as follows[3, 4, 5, 6, 7, 8, 9] :
Even with optimal clinical, radiographic, and histologic data, there is often no clear distinction between benign and low-grade malignant cartilage tumors.[1, 12, 13, 14] This distinction is particularly difficult with very-low-grade chondrosarcomas, or so-called borderline chondrosarcomas. These cartilage tumors have cytology resembling enchondromas; cortical erosions or scalloping without frank full-thickness cortical destruction visible on plain radiographs; clinical presentation of intermittent to constant pain; and local recurrences similar to those of low-grade chondrosarcomas.[15, 16]
Low-grade malignant chondrosarcomas, which constitute the majority of malignant cartilage tumors, have been described as having a slow growth rate, infrequent metastases, and a 90% 5-year survival rate.[1, 2, 17]
In addition to the conventional intramedullary tumors, both benign and malignant cartilage tumors may be found in periosteal locations or in soft tissue. Secondary chondrosarcomas may arise in an osteochondroma, in an enchondroma, or in the setting of enchondromatosis (Ollier disease or Maffucci syndrome) or multiple osteochondromatosis. The secondary chondrosarcomas are more likely to occur in patients with multiple cartilage tumors and typically present as a painful, progressively enlarging bony mass. Dedifferentiated chondrosarcoma is a distinct subgroup of chondrosarcoma in which a high-grade noncartilaginous sarcoma is adjacent to either a low-grade chondrosarcoma or enchondroma.
Lee et al monitored 227 patients with chondrosarcoma for an average of 6 years and reported predictive factors for metastasis to be local recurrence, pelvic location, tumor volume greater than 100 cm3, aneuploidy of the tumor coupled with a high mean DNA index, histologic grade 3, and dedifferentiated chondrosarcomas. The reported recurrence rate ranges from 4% to 12%, depending on initial treatment modality and tumor grade.[18, 19]
Classically, because chondrosarcomas are known to be resistant to radiotherapy and chemotherapy, wide resection has generally been accepted as recommended treatment for low-grade chondrosarcoma.[20, 21, 22, 23, 24, 25] Borderline cartilage tumors have an even lower metastatic potential than the true low-grade (grade 1) malignant chondrosarcoma.[11, 15] Thus, recommended treatment of these borderline tumors has ranged from marginal curettage and grafting to limited local resection.
There has been a push for more conservative treatment of borderline and low-grade malignant chondrosarcomas, with extended intralesional curettage being considered a viable alternative to wide resection.[11, 15, 16, 26]
NextThe following discussion is a description of 2 cases that initially presented as clinically, radiographically, and pathologically borderline cartilage tumors and eventually demonstrated aggressive metastatic behavior, as well as a third case in which a radiographically and histologically benign enchondroma was detected only after it had undergone dedifferentiation into a high-grade osteosarcoma and resulted in a pathologic fracture.
A 38-year-old female athlete presented with a minimally painful lump on the medial side of her left knee (see the first image below). She underwent open biopsy with curettage later that same month. Histology at that time showed benign enchondroma with focal atypia (see the second image below). The patient developed a recurrence of the mass 19 months later. She underwent augmented (phenol) marginal resection 2 months after the recurrence, after refusing wide resection. Histology showed progression from a purely low-grade to a mixed low- and intermediate-grade lesion (ie, chondrosarcoma grade 1-2 of 3 [see the third image below]).
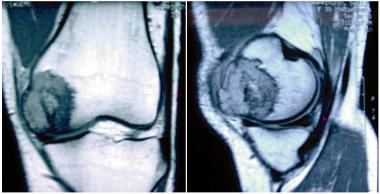 Original MRI of a patient demonstrating a lesion extending beyond the boundary of normal bone.
Original MRI of a patient demonstrating a lesion extending beyond the boundary of normal bone.
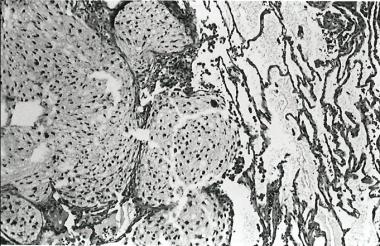
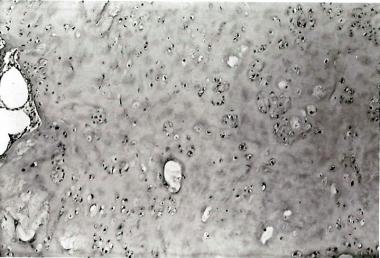 Histology of original lesion demonstrating what was thought to be a benign enchondroma with some atypical features.
Histology of original lesion demonstrating what was thought to be a benign enchondroma with some atypical features.
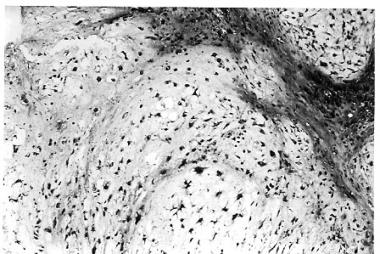 Recurrent tumor demonstrating progression from a purely low-grade lesion to a mixed low- and intermediate-grade lesion.
Recurrent tumor demonstrating progression from a purely low-grade lesion to a mixed low- and intermediate-grade lesion.
One year after the first recurrence, she developed a second recurrence and underwent wide resection and reconstruction of the distal femur. The tumor within the distal femur was a high-grade dedifferentiated chondrosarcoma with osteosarcomatous features (see the image below). She then underwent adjuvant chemotherapy for osteosarcoma.
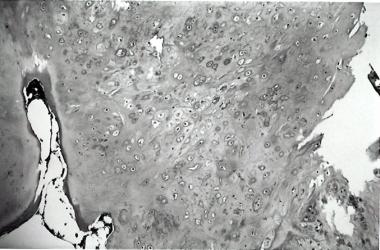
 Tumor from distal femur at time of reconstruction demonstrating dedifferentiated chondrosarcoma.
Tumor from distal femur at time of reconstruction demonstrating dedifferentiated chondrosarcoma.
Five months after the second recurrence, she developed lung metastases. Biopsy of the lung lesions revealed dedifferentiated chondrosarcoma. One month later, she developed a recurrence of the high-grade sarcoma in the popliteal fossa. The patient underwent above-knee amputation and died of progression of the lung metastases 1 year later.
A 39-year-old man presented with anterior bowing of his right femur and a leg-length discrepancy. At age 16 years, he had undergone an osteotomy to correct the angular deformity. Plain radiography of the right distal femur revealed a cartilage tumor in the distal femur. MRI demonstrated disruption of the anterior femoral cortex, with thinning of the articular cartilage. The patient underwent curettage and bone grafting. Histologic examination revealed a well-differentiated cartilaginous tumor, and a diagnosis of benign enchondroma was favored (see the first image below). The original osteotomy was apparently through the enchondroma (see the second image below).
 Tumor from pin sites revealing a well-differentiated cartilaginous tumor. The diagnosis of benign enchondroma was favored at this point.
Tumor from pin sites revealing a well-differentiated cartilaginous tumor. The diagnosis of benign enchondroma was favored at this point.
 AP radiograph of the knee demonstrating a tumor around screw holes.
AP radiograph of the knee demonstrating a tumor around screw holes.
The patient reported recurrent knee pain 20 months after curettage and bone grafting and underwent repeat curettage. The histology showed progression to grade 2 chondrosarcoma (see the image below). Follow-up CT scan showed a lytic lesion in the posterior femoral condyle extending to the distal femoral joint line. He underwent wide resection with distal femoral replacement 2 months later. The histologic examination confirmed grade 2 chondrosarcoma.
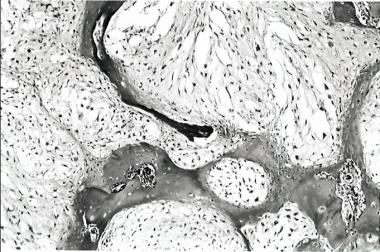 Histology at time of recurrence showing progression to grade 2 chondrosarcoma.
Histology at time of recurrence showing progression to grade 2 chondrosarcoma.
Thirteen months later, CT scanning of the chest revealed approximately 20 small pulmonary nodules. The resected lung nodules all revealed grade 2 chondrosarcoma histologically identical to the tumor excised from the distal femur (see the image below). The patient initiated chemotherapy. Six months later, he had multiple enlarging nodules but remained asymptomatic, and he refused further treatment.
 Histology showing grade 2 chondrosarcoma within lung metastases. This tumor was identical to the tumor resected from the distal femur.
Histology showing grade 2 chondrosarcoma within lung metastases. This tumor was identical to the tumor resected from the distal femur.
A 70-year-old man sustained a right supracondylar femur fracture after stepping out of the bathtub. Incisional biopsy of the fracture site was performed. Histologic examination revealed a high-grade osteosarcoma with soft tissue extension sharply juxtaposed to an enchondroma (see the image below). He underwent right hip disarticulation 1 week later. He declined chemotherapy. Lung nodules appeared on chest radiography 2 months postoperatively. CT scanning confirmed the presence of multiple pulmonary nodules consistent with metastases.
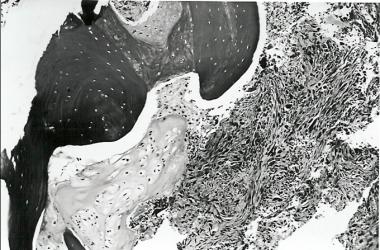
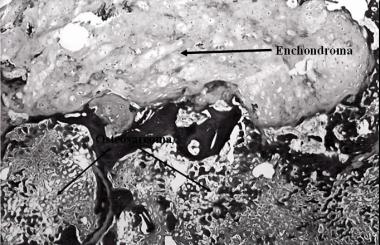 Histology at fracture site demonstrating sharp juxtaposition of benign enchondroma with osteosarcoma.
Histology at fracture site demonstrating sharp juxtaposition of benign enchondroma with osteosarcoma.
Differentiation of benign active and low-grade (grade 1) malignant cartilaginous lesions is difficult. Recent diagnostic schemata have included a borderline category of cartilage tumors.[15, 16] Some authors have supported a more conservative intralesional curettage with or without surgical adjuvant therapy (such as liquid nitrogen or phenol) as effective therapy for these borderline tumors. Although the overall recurrence rate of low-grade chondrosarcoma is low, a substantial proportion of the recurrent tumors manifest themselves at a higher histologic grade than their corresponding primary tumors. The reported frequency of this recurrence varies in the literature but may be as high as 61%.[19]
Case 1 and Case 2 are examples of grade progression from a borderline tumor to a grade 2 chondrosarcoma. Both patients underwent limited resection of their original borderline chondrosarcomas, but the disease recurred as higher-grade tumors at 19 and 20 months from initial presentation, respectively. The patient in Case 1 refused wide resection at recurrence and eventually developed lung metastases after dedifferentiation at the primary site. Whether this poor outcome could have been prevented with wide resection of the recurrent tumor is unknown. The patient in Case 2, on the other hand, did undergo wide resection of recurrent tumor, but metastasis occurred nevertheless. Although both cases underscore the need for wide resection of the recurrent chondrosarcoma, the second case questions the safety of conservative management for borderline chondrosarcoma.
Case 3 is an example of what appeared to be a solitary benign enchondroma that dedifferentiated into a high-grade osteosarcoma. This is a rare event, with only a few cases reported in the literature.[27] Although wide excision would not be the recommended treatment for a benign enchondroma, this case serves as another example of an unusually aggressive cartilage tumor.
Currently, no prospective, controlled studies describe the appropriate treatment for borderline or low-grade (grade 1) malignant chondrosarcomas. Some authors have suggested that extended intralesional curettage may be acceptable for both types. However, limited resection was clearly insufficient to control borderline cartilage tumors in the case studies described above and resulted in an unexpectedly poor outcome. Caution should be utilized both in making the distinction between benign and malignant cartilage tumors and in selecting the appropriate surgical treatment for grade I chondrosarcomas.
Copyright © www.orthopaedics.win Bone Health All Rights Reserved