The current main techniques of Posterior Lumbar Interbody Fusion (PLIF) surgery all incorporate a supplementary intervertebral implant:
• Threaded cylindrical cages made of titanium, cortical allograft (donor bone) or synthetic bone.
• Impacted cages made of titanium, carbon-fiber reinforced or plain PEEK polymer (Polyetheretheketone).
• Impacted wedges made of carbon-fiber reinforced PEEK, plain PEEK polymer or cortical allograft.
• Inserted and rotated wedges made of carbon-fiber reinforced PEEK or plain PEEK polymer.
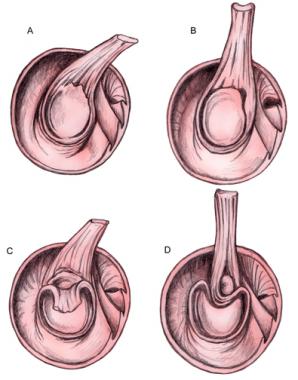
They all involve an initial laminectomy and a variable amount of removal of the facet joints (medial facetectomy). The latter, which may require complete removal of the facet joints, will depend upon the choice and size of implant, as well as the surgical level. Following decompression of the spinal canal, intervertebral disc space spreaders are used to correct coronal plane deformity (scoliosis) and restore disc space and foraminal height (Figure 2).
Figure 2. Restoration of disc space height with
intervertebral spreaders usually reduces slip by ~ 50%
Supplementary pedicle screw instrumentation may then be used to complete the correction of any spondylolisthetic deformity (spondylolisthesis) (Figures 3 and 4).
Figure 3. Spondylolisthesis reduction using a screw
thread to apply a powerful posterior translation force.
Figure 4. Complete reduction and PLIF
in a 15 year old boy with Grade III spondylolisthesis
Most modern techniques rely on supplementary pedicle screw instrumentation to assist the stabilization / deformity correction although some surgeons still regard the distraction (separation)/ compression stabilization achieved by the implants to be satisfactory.
In the case of threaded cylindrical cages, bilateral holes are then made, centered upon the disc space and removing several millimeters of the adjacent vertebral end plates. The holes are tapped and the implants, filled with bone graft are screwed into the holes. Care must be taken to avoid injury to the adjacent nerve roots during preparation of the holes and implantation of the cages as these devices.
With impacted cages / wedges, the posterior disc space is usually over-distracted (separated) to enable an implant of sufficient anterior height to be inserted. A broach (a surgical instrument) may be used to prepare a path through the posterior disc space. The disc space contents and cartilaginous end plates are removed to facilitate fusion. In the case of impacted wedges, bone graft is after loaded into the disc space beside the wedges.
The Insert and Rotate technique is similar to the Impacted wedge technique but does not require over-distraction (separation) or involve the cutting of any channel through the posterior end plates. It separates the load bearing and stabilization role from the fusion role. The bone graft is after loaded and placed to either side of the implants. The implant may be made quite lordotic to facilitate restoration of Lordosis (natural inward spinal curvature), especially of the lumbosacral (lumbar / sacrum) segment. Care must be taken to preserve the vertebral end plates upon which the implant will rest. It requires minimal dural / neural retraction (Figure 5). Supplementary pedicle screw instrumentation must be used.
Figure 5. Schematic representation of the difference in the neural retraction
required for Threaded Cylindrical, Impacted and Insert and Rotate implant techniques.
Both the Impacted and Insert and Rotate techniques are suitable for use with minimal access techniques.
Copyright © www.orthopaedics.win Bone Health All Rights Reserved