Coronoid fractures are often seen as a part of complex elbow fracture dislocations or high Monteggia fractures (rare).
NextFractures of the coronoid rarely occur in isolation. They usually occur in combination with a radial head fracture, a dislocation of the elbow, or both (terrible triad of the elbow).[1] Large coronoid fractures often are associated with persistent elbow instability even after reduction of the dislocation. Recently, the trend has been toward fixation of these injuries to restore stability and initiate an early range-of-motion program.[2, 3, 4, 5, 6, 7]
Images depicting the elbow joint can be seen below.
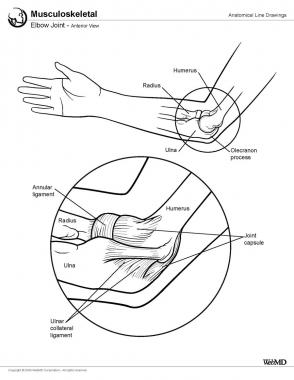 Elbow joint, anterior view.
Elbow joint, anterior view.
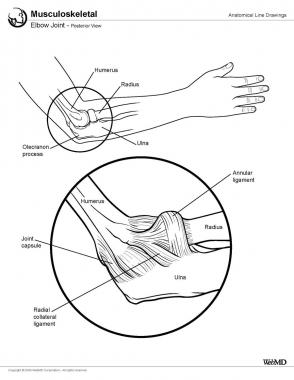 Elbow joint, posterior view.
Elbow joint, posterior view.
Coronoid fractures account for less than 1-2% of all elbow fractures. Coronoid fractures have been identified in 10-15% of elbow dislocations.[8, 9] Radial head fractures are seen in about 5-10% of elbow dislocations.[10] Coronoid fractures, especially with large fragments, are associated with more instability and an increased incidence of complications.
Coronoid fractures were believed to result from avulsion of a bony fragment of the coronoid by the brachialis, which inserts onto the coronoid process. This, however, does not explain the mechanism of type 1 and some type 2 fractures, as the brachialis attaches to the base of the coronoid process of the ulna. (See Workup, Imaging Studies, below, for a discussion of fracture types.) These fractures probably occur from shear forces at the time of the dislocation when the trochlea pushes off a piece of the coronoid.
Morrey and coworkers, in their biomechanical study of the elbow, concluded that approximately 50% of the elbow stability comes from the congruent articulation between the trochlea and the ulna.[11]
Closkey et al studied the stabilizing function of the coronoid process under axial load to the elbow.[12] They found no significant difference, at any flexion position, in posterior axial displacement between intact elbows and elbows in which 50% or less of the coronoid process was fractured (types 1 and 2) (P = .43). Differences in posterior axial displacement were significant, across all flexion positions, between intact elbows and elbows in which more than 50% of the coronoid process was fractured (type 3) (P = .006). They concluded that in response to axial load, elbows with a fracture involving more than 50% of the coronoid process displace more readily than elbows with a fracture involving 50% or less of the coronoid process, especially when the elbow is flexed 60º and beyond.
Coronoid fractures are usually seen in patients with elbow dislocations. The patient usually presents with a history of a fall on the outstretched hand and a deformity of the elbow.
The presence of an unstable reduction is suggestive of an associated coronoid or radial head fracture. An irreducible dislocation, on the other hand, should arouse suspicion of soft tissue (brachialis, median nerve) or bony (medial epicondyle) interposition in the joint.
Distal vascularity and neurologic status should always be tested in these cases.
In children, coronoid fractures have a bimodal age distribution, with peaks at age 8-9 years and at age 12-14 years.[13] Coronoid fractures in children are often associated with elbow dislocations, olecranon fractures, medial epicondyle fractures, or lateral condyle fractures.
In children younger than 6 years, Blasier has described an unusual flap injury of the unossified coronoid in which the elbow is dislocated and a small flap of the articular surface gets flipped back into the joint.[14] This usually appears on the lateral radiograph as a small flake of bone in the anterior portion of the joint. This flake is a clue to the underlying pathoanatomy and the extent of injury.
A displaced coronoid fracture that presents with a block to elbow motion is a definite indication for surgical stabilization.[15]
Type 3 fractures need to be fixed.[16] If the fragment is too comminuted for internal fixation, then a hinged external fixator should be applied across the elbow and a protected range-of-motion program should be started.[17] Type 2 fractures with elbow instability are also best treated with a hinged external fixator.
Giannicaola et al studied 18 patients in whom coronoid fractures were repaired using fine-threaded K-wires. After 26 months, results were excellent in 10 patients, good in 7, and fair in 1, according to the Mayo Elbow Performance Index. The authors concluded that this technique was an easy, minimally invasive, stable, and successful procedure for obtaining osteosynthesis in patients with coronoid fractures and complex elbow instability.[18]
Type 1 and most type 2 fractures are usually managed nonoperatively.[19]
The coronoid acts as the anterior buttress of the greater sigmoid notch of the ulna. It provides attachment to the anterior band of the medial collateral ligament (MCL) and the middle portion of the anterior capsule. The anterior colliculus of the MCL is the primary stabilizer of the elbow against valgus strain in the functional arc of 20-120° of flexion. This ligament is most likely to become injured with a low coronoid fracture with the elbow in full extension.[20] A fracture of the coronoid, therefore, results in the loss of all of these supports. The brachialis muscle is attached to the base of the coronoid process.[21] Dissection of the brachialis during fixation of these fractures contributes to the risk of heterotopic ossification in these cases.
Type 1 and type 2 fractures usually do not require operative stabilization.[22] Highly comminuted type 3 fractures pose a significant problem during open reduction and internal fixation (ORIF) and may be better treated with a hinged external fixator.[23]
Gray et al studied the effect of a prosthesis on restoring stability to the coronoid-deficient elbow by analyzing 8 cadaveric arms. Researchers concluded that the use of an anatomical implant restores stability and deserves further study.[24]
Workup
Copyright © www.orthopaedics.win Bone Health All Rights Reserved


