QuestionQUESTION: I am a 44 year old female and just recently started visiting a chiropractor to get
relief from headacahes and Fibromyalgia symptoms; stiffness and cramping.
After the initial few visits, I felt a "good" soreness, but when he made neck
adjustments for subluxation, I would feel a strain. After the 5th visit in 3 weeks,
I experienced a terrible migraine and a burning pain in my upper back that goes
all the way down to the bottoms of both feet. I feel a little dizzy and can't get
relief from the burning sensation, yet I don't have a fever. My neck is very sore,
particularly in the back of the head and on both sides. I am having trouble
sleeping and the pain goes up through my skull to right between the eyes. My
scalp feels raw. Lastly, I am having a twitching in my pinky on my left hand and
the inside of both ears are burning. The most troublesome part is the fire in my
spine and in my shoulders blades. I am currently taking 60mg of Prozac daily
and recently started taking Ambien to help me sleep (5mg), with no benefit so I
don't intend to take Ambien anymore. I also take Advil regularly for cramping
and pain, but the Advil is having no affect on the burning. Although I've suffered
with Fibromyalgia, IBS, Endometriosis, and frequent headaches for over 2 years, I
have NEVER felts this awful burning pain before! Even my inner organs are
burning. Since it is the weekend, I will go see my regular doctor on Monday if I
am not feeling better. I am 99% sure that I will not be going back to the
chiropractor. I am considering going to urgent care or emergency, but they are
less than helpful unless you are dying. Am I? I am desperate for advice as to
what I am experiencing. Thanks in advance.
ANSWER: Dear Angel,
You should probably print this out, it is lengthy. Feel free to share it with your doctors.
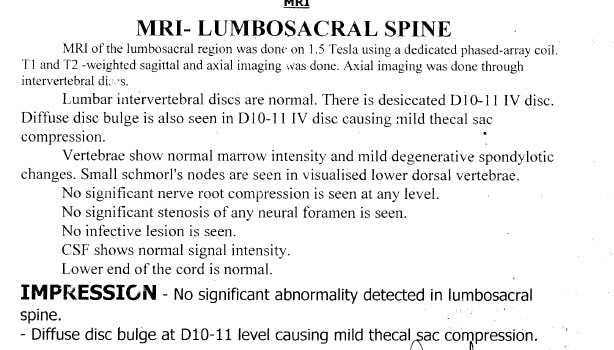
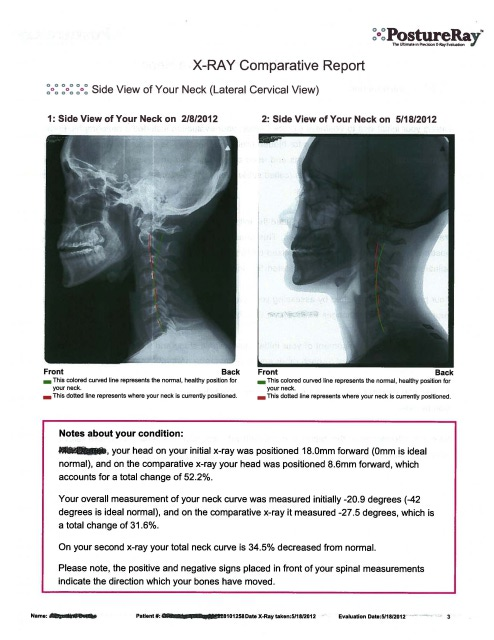
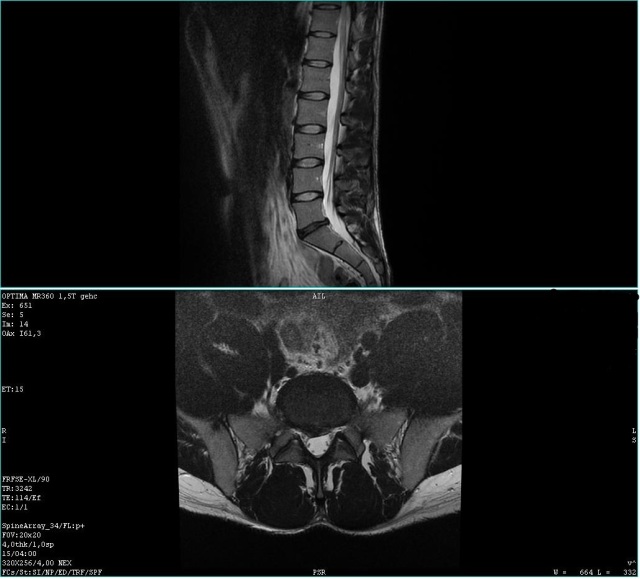
I must first ask, did the chiropractor perform an orthopedic examination of your neck, with measured range of motion, physical functional testing, neurological testing, deep tendon reflexes, and x-rays of the spine? I hope so. Anyway with your history it is expected that you would be sore and have muscular strain after the adjustments, but the burning pain experienced is not a normal response...did you tell the chiropractor this was occurring? He/she should be made aware of it immediately, and your symptoms warrant the ordering of an MRI of the neck and upper back, especially if they are not improving. There is something called a long tract sign that could be occurring. Basically this is where the spinal cord is irritated in the neck which causes pain transmission and altered signals to be send down the spinal cord. Possible chemical and anatomical irritants: disk bulge/herniation, histological inflammation, spinal stenosis, syrinx formation...MRI can evaluate all of these things, while x-rays have limited value concerning the soft tissue structures.
There are a few things that may have occurred: The first and most likely is that the chiropractor flared up the fibromyalgia and this has shifted into overdrive...Fibromyalgia is really just an overactive pain response generated by the lack of oxygenation to the tissues and when muscles are overstimulated by stretch or movement, the pain can be significantly increased. Second the vagus nerve could have been hyper-stimulated by the neck adjustment due to the connections with the trigeminal ganglion and the upper cervical complex in the neck. Normally this is a good thing, however in your condition, it may have aggravated symptomatology. The vagus nerve sends information to the organ systems in the chest and abdominal cavity. Upper cervical stimulation can also affect the cranial nerves that send information to the ear (vestibulocochlear nerve). Third, the lower cervical nerve roots may have become inflamed or experienced some compression which would account for the twitching in the pinkies (ulnar nerve distribution). Lastly, and the most remote possibility, the chiropractor could have actually damaged some tissue in the neck such as the musculature, or the disc, but this is very rare...and if the disc was damaged, it was probably already so, and the adjustment only flared it up. The clinical literature is pretty clear on these matters and there is very little risk for any type of damage to the spinal structures with chiropractic care. You should really call the office and speak directly with the doctor so this can be documented in your file.
Concerning your primary medical doctor, they are not likely to do anything for you other than write you a script for pain meds or muscle relaxers and refer you to a neurologist, however, if he/she orders an MRI, this could be very helpful in determining if there are any intrinsic problems with the spine. Lastly, I am going to send you some detailed information on clinical research concerning your fibromyalgia...I think this is likely the main issue at hand, and most fibomyalgia patients are not managed well by chiropractors or medical doctors. See below.
Respectfully,
Dr. J. Shawn Leatherman
www.suncoasthealthcare.net
Management of Fibromyalgia: Rationale for the use of Magnesium and Malic Acid: Journal of Nutritional Medicine No. 3, 1992, pp. 49-59
Guy E. Abraham MD and Jorge D. Flechas MD, MPH
FROM ABSTRACT:
Primary Fibromyalgia (FM) is a common condition affecting mainly middle-aged women. Of the etiologies previously proposed, chronic hypoxia seems the one best supported by recent biochemical and histological findings.
We postulate that FM symptoms are predominantly caused by enhanced gluconeogenesis with breakdown of muscle proteins, resulting from a deficiency of oxygen and other substances needed for ATP synthesis. We present data supporting a critical role for magnesium and malate in ATP production under aerobic and hypoxic conditions; and indirect evidence for magnesium and malate deficiency in FM.
After treating 15 FM patients for 8 weeks with an oral dose between 1200-2400 mg of malate and 300-600 mg of magnesium, fibromyalgia tender point scores were reduced by about 60% at 4 weeks and 66% at 8 weeks. Subjective improvement of myalgia occurred within 48h of supplementation. [WOW]
THESE AUTHORS ALSO NOTE:
揊ibromyalgia (FM) is a common clinical syndrome of generalized musculoskeletal pain, stiffness and chronic aching, characterized by reproducible tenderness on palpation of specific anatomical sites, called tender points.?
--FM is primary when not associated with systemic causes, trauma, cancer, thyroid diseases and pathologies of rheumatic or connective tissues.
--揊M is nine times more common in middle-aged women (between the ages of 30 and 50 years) than in men.?
--FM is one of the most common rheumatic complaints with clinical prevalence of 6%-20%.
--FM is associated with irritable bowel syndrome, tension headache, primary dysmenorrhea, mitral valve prolapse and chronic fatigue syndrome.
--Various treatment modalities have been tested in FM patients with poor results, including tryptophan, ibuprofen, and tricyclic drugs.
--揈levated catecholamines are observed in urine of FM patients.?[IMPORTANT FOR CHIROPRACTORS]
--Hypoxia is postulated to play an etiologic role in the development and the symptoms of FM.
There is evidence that fibromyalgia is a result of deficiencies of substances needed for ATP synthesis. The synthesis of proteins, fats and carbohydrates is dependent on ATP availability, which supplies the energy for their synthesis and actions. The synthesis of ATP by the mitochondria requires the presence of oxygen, magnesium, substrate [food], ADP, and inorganic phosphate (phosphate). When all substances are present in optimal concentrations, the integrity of the mitochondrial membrane and the capacity of the enzymatic system in the respiratory chain become the rate-limiting factor in the synthesis of ATP.
The five ingredients required for the synthesis of ATP are:
1) Oxygen
2) Magnesium
3) Substrate [food]
4) ADP
5) Inorganic phosphate
Therefore, the synthesis of ATP is reduced by reduction of any of the 5 ingredients, as follows:
1) Oxygen is reduced by hypoxia, magnesium deficiency, and malate deficiency.
2) Magnesium is reduced by excess aluminum and/or excess calcium.
3) Substrate is reduced by malnutrition.
4) ADP is reduced by phosphate deficiency and/or magnesium deficiency.
5) Inorganic phosphate is reduced by magnesium and/or malate deficiency or from excess calcium and/or aluminum.
Additionally, the capacity of the respiratory chain to produce ATP is controlled by the vitamins thiamine (B1), riboflavin (B2), and pyridoxine (B6) because they are essential for the electron transport system. 揂ll three vitamins require a magnesium dependent phosphate transfer reaction to become biologically active.?br>
Lastly, the production of ATP is dependent upon mitochondrial membrane integrity. 揗agnesium deficiency causes mitochondrial swelling, increased membrane permeability and uncoupling of oxidative phosphorylation.?br>
Therefore, magnesium and malate play a pivotal role in mitochondrial membrane integrity, mitochondrial respiration and oxidative phosphorylation in the production of ATP.
During anaerobic glycolysis, from glucose to acetyl-Co A, there are 11 distinct steps; 9 of 11 [82%] steps require magnesium. The Krebs Cycle (Citric Acid Cycle) has 9 steps, and 3 [30%] of them require magnesium: [IMPORTANT]
Anaerobic glycolysis delivers 2 moles of ATP per mole of glucose whereas aerobic glycolysis to carbon dioxide and water through the citric acid cycle delivers 36-38 moles of ATP per mole of glucose. 揟herefore, adequate oxygen supply enhances ATP yield by 18-19 fold.?br>
揜elative hypoxia has been demonstrated in FM patients; and FM symptoms improved following aerobic conditioning.? 揗agnesium plays a critical role in key enzymatic reactions for both aerobic and anaerobic glycolysis.?
揟he uptake and accumulation of magnesium by mitochondria is associated with enhanced uptake of phosphate and proton extrusion. The uptake of phosphate is required for phosphorylation of ADP, and the proton extrusion is the driving force in the oxidative phosphorylation of ADP.?br>
揂luminum inhibits glycolysis and oxidative phosphorylation with decreased intra-mitochondrial ATP levels.?br>
Aluminum has a high affinity for phosphate groups and therefore blocks the absorption and utilization of phosphate for ATP synthesis, causing an intramitochondrial phosphate deficiency. Adequate levels of magnesium prevent this toxic effect of aluminum. Malic acid is one of the most potent chelators of aluminum and most effective in decreasing brain aluminum levels.
Both magnesium and malate improve the efficiency of oxygen utilization in producing ATP. Magnesium and malate deficiency induce a relative hypoxia.
There is evidence of magnesium deficiency in FM patients. 揗agnesium deficiency causes swelling and disruption of cristae in mitochondria, with a decreased number of mitochondria per cell.? These mitochondrial abnormalities have been reported in muscle biopsies of tender points obtained from FM patients.
揟he most common symptoms associated with FM梞yalgia, chronic fatigue syndrome, irritable bowel syndrome, mitral valve prolapse, tension headache and dysmenorrhea 梙ave been reported in patients with magnesium deficiency, and magnesium supplementation improves these symptoms.?br>
Malate plays an important role in generating mitochondrial ATP. Three moles of ATP are formed for each mole of malate oxidized to oxaloacetate.
揙nly tissue malate is depleted following exhaustive physical activity, in spite of the fact that the other key metabolites from the citric acid cycle necessary for ATP production remain unchanged.?The malate deficiency is the cause of the physical exhaustion.
揗alate acts as an electron donor and generates a large proton motive force, believed to be the driving force for the mitochondrial synthesis of ATP.? 揜elatively small amounts of exogenous malate are required to increase mitochondrial oxidative phosphorylation and ATP production.?br>
揢nder hypoxic conditions, there is an increased demand for malate because malate is not only oxidized to oxaloacetate but also reduced to succinate. 揗alate is the only metabolite of the citric acid cycle which correlates positively with physical activity.?br>
揑n humans as well as in other animals tested, when there is increased demand for ATP, there is also an increased demand and utilization of malate.?br>
Vitamin B6 and magnesium are required for normal activity of malate dehydrogenases, [the Kreb抯 Cycle enzyme that catalyzes the conversion of malate into oxaloacetate (see picture)]. A deficiency of malate dehydrogenases creates a relative malate deficiency in fibromyalgia patients. Thyroid hormones stimulate malate dehydrogenases, and therefore help fibromyalgia patients.
Respiratory chain ATP synthesis requires adequate amounts of the vitamins thiamine and riboflavin, which are the precursors of NAD and FAD [required for electron transport] respectively.
Vitamins thiamine (B1), riboflavin (B2), and pyridoxine (B6), require a magnesium-dependent phosphate transfer reaction to become biologically active. 揗agnesium deficiency would therefore create a sluggish respiratory chain and a decreased efficiency in the transfer of reducing equivalents from the cytosol to the mitochondria.?br>
**Malate demands are greater in hypothyroid fibromyalgia patients.**
揂DP deficiency has been reported in muscle biopsies of tender points obtained from FM patients.?The following are known to cause mitochondrial ADP deficiencies:
1) Mitochondrial ADP deficiency occurs if magnesium concentrations are below optimal levels.
2) Mitochondrial ADP deficiency occurs if phosphate concentrations are below optimal levels.
3) The mitochondrial uptake of phosphate depends on malate levels: required for exchange with phosphate.
4) The uptake of phosphate is also enhanced by the uptake and accumulation of magnesium by mitochondria.
5) **Intra-mitochondrial phosphate deficiency occurs in the presence of low levels of magnesium and malate.
6) Excess calcium and aluminum also predispose to intra-mitochondrial phosphate deficiency.
揗agnesium plays an important role in the integrity of the mitochondrial membrane. Magnesium deficiency is associated with swelling of the mitochondria; increased permeability and decreased selectivity of mitochondrial inner membrane and uncoupling of oxidative phosphorylation.?揂bnormalities of mitochondrial membranes have been reported in FM patients.?br>
In this study, 15 patients (age 32-60) with a diagnosis of fibromyalgia based on the American College of Rheumatology criteria were supplemented with a total daily dosage of 300-600mg of elemental magnesium and 1200-2400 mg of malic acid. 揂ll patients reported significant subjective improvement of pain within 48 h of starting.?br>
DISCUSSION FROM SUNCOAST HEALTHCARE PROFESSIONALS
Oxygen is required to make ATP. Chronic hypoxia results in reduction of ATP. The body will respond by increasing anaerobic glycolysis, resulting in increased pyruvate production and increased lactic acid, both of which increase pain perception. The pain of fibromyalgia is caused in part by hypoxia (which is in itself painful) and the increase of lactic acid from increased anaerobic glycolysis.
Glucose is also required to make ATP. Therefore, the body will also respond by attempting to increase the genesis of glucose. The body can make glucose for the purpose of producing ATP by assembling it from smaller molecules, especially from amino acids. The process of assembling glucose from smaller molecules is termed gluconeogenesis. To make glucose from amino acids, the body has to breakdown proteins, a process termed proteolysis, and the best source of protein for this purpose is from the muscles. The pain of fibromyalgia is also caused by the proteolysis of muscle tissue that occurs in order for the required gluconeogenesis to increase ATP synthesis in these patients.
KEY POINTS FROM SUNCOAST HEALTHCARE PROFESSIONALS
1) 揊ibromyalgia (FM) is a common clinical syndrome of generalized musculoskeletal pain, stiffness and chronic aching, characterized by reproducible tenderness on palpation of specific anatomical sites, called tender points.?
2) Fibromyalgia is primary when not associated with systemic causes, trauma, cancer, thyroid diseases and pathologies of rheumatic or connective tissues.
3) 揊M is nine times more common in middle-aged women (between the ages of 30 and 50 years) than in men.?br>
4) The best proposed etiology for fibromyalgia is chronic hypoxia.
5) These authors propose that fibromyalgia symptoms are predominantly caused by enhanced gluconeogenesis with breakdown of muscle proteins, resulting from a deficiency of oxygen and other substances needed for ATP synthesis.
6) Magnesium and malate have a critical role in ATP production and therefore fibromyalgia symptoms may be caused by magnesium and malate deficiency.
7) Fibromyalgia is associated with irritable bowel syndrome, tension headache, primary dysmenorrhea, mitral valve prolapse and chronic fatigue syndrome.
8) Various treatment modalities have been tested in FM patients with poor results, including tryptophan, ibuprofen, and tricyclic drugs.
9) 揈levated catecholamines are observed in urine of FM patients.?[Important: elevated catecholamines (norepinephrine and epinephrine) are the result of increased sustained sympathetic tone. Increased sustained sympathetic tone can be the consequence of reduced mechanical integrity, such as a vertebral fixation]
10) Reduced oxygen reduces ATP synthesis. Hypoxia, magnesium deficiency and malate deficiency reduce ATP.
11) Magnesium is reduced by excess aluminum and/or excess calcium.
12) ATP production is controlled by the vitamins thiamine (B1), riboflavin (B2), and pyridoxine (B6) because they are essential for the electron transport system, and all three vitamins require magnesium to become biologically active.
13) During anaerobic glycolysis, from glucose to acetyl-Co A, there are 11 distinct steps; 9 of 11 [82%] steps require magnesium.
14) The Krebs Cycle (Citric Acid Cycle) has 9 steps, and 3 of them [30%] require magnesium:
15) An 揳dequate oxygen supply enhances ATP yield by 18-19 fold.?br>
16) Fibromyalgia symptoms improve following aerobic conditioning.
17) Aluminum has a high affinity for phosphate and blocks the absorption and utilization of phosphate for ATP synthesis, causing decreased mitochondrial ATP levels. Adequate levels of magnesium prevent this toxic effect of aluminum.
18) Malic acid is one of the most potent chelators of aluminum and is most effective in decreasing brain aluminum levels.
19) 揟he most common symptoms associated with FM梞yalgia, chronic fatigue syndrome, irritable bowel syndrome, mitral valve prolapse, tension headache and dysmenorrheal 梙ave been reported in patients with magnesium deficiency, and magnesium supplementation improves these symptoms.?br>
20) Malate deficiency is the cause of the ATP deficiency seen with exhaustive physical activity.
21) 揑n humans as well as in other animals tested, when there is increased demand for ATP, there is also an increased demand and utilization of malate.?
22) Malate demands are greater in hypothyroid fibromyalgia patients.
23) Fibromyalgia patients supplemented with a daily dose of 300-600 mg magnesium plus 1200-2400 mg of malic acid -- 揳ll patients reported significant subjective improvement of pain within 48 h of starting.?Additionally, the fibromyalgia tender point scores were reduced by about 60% at 4 weeks and 66% at 8 weeks.
COMMENTS FROM SUNCOAST HEALTHCARE PROFESSIONALS
The malic acid plus magnesium supplement Suncoast uses in the management of fibromyalgia patients is: Complete FM from Nutri-West: Each capsule contains 294 mg of malic acid and 59 mg of magnesium.
Each capsule also contains a balance of compounds that have also been shown to benefit patients with fibromyalgia: grapeseed extract, betatine HCL, silymarin extract, bromelain, papain, trypsin, lipase, amylase, pancreatin, lecithin (phosphytidal choline), l-leucine, l-valine, glucosamine sulfate, N-acetyl glucosamine, and ornithine alpha keto-glutarate.
Another article [Treatment of fibromyalgia syndrome with Malic Acid: Journal of Rheumatology, May 1995;22(5):953-8] suggests that the minimum dosage of Complete FM should be 6 tablets per day (2 with each meal), which would supply: 1,764 mg of malic acid and 354 mg of magnesium . For some patients, the optimal dosage needs to be increased to 9 tablets per day (3 with each meal), supplying: 2,646 mg of malic acid and 531 mg of magnesium.
Effects of muscle strengthening versus aerobic exercise program in fibromyalgia: Rheumatology International, November 3, 2007
? Bircan, S. A. Karasel, B. Akg黱, ? El ?S. Alper
FROM ABSTRACT
The purpose of this study was to compare the effects of aerobic training with a muscle-strengthening program in patients with fibromyalgia. Thirty women with fibromyalgia were randomized to either an aerobic exercise (AE) program or a strengthening exercise (SE) program for 8 weeks.
Outcome measures included the intensity of fibromyalgia-related symptoms, tender point count, fitness (6-min walk distance), hospital anxiety and depression (HAD) scale, and short-form health survey (SF-36).
There were significant improvements in both groups regarding pain, sleep, fatigue, tender point count, and fitness after treatment. HAD-depression scores improved significantly in both groups while no significant change occurred in HAD anxiety scores.
Bodily pain subscale of SF-36 and physical component summary improved significantly in the AE group, whereas seven subscales of SF-36, physical component summary, and mental component summary improved significantly in the SE group.
When the groups were compared after treatment, there were no significant differences in pain, sleep, fatigue, tender point count, fitness, HAD scores, and SF-36 scores. AE and SE are similarly effective at improving symptoms, tender point count, fitness, depression, and quality of life in fibromyalgia.
THESE AUTHORS ALSO NOTE:
揊ibromyalgia is a chronic painful condition characterized by widespread pain, pain at specific tender points, sleep disturbance, and fatigue.? Fibromyalgia is more common in females than males.
The symptoms of fibromyalgia are often caused by altered peripheral nociceptive mechanisms and central pain processing. [wind-up, central sensitization]
揑t is widely accepted that exercise is beneficial for patients with fibromyalgia.?& 揟he majority of patients with FM are known to be aerobically unfit and have poor muscle strength and limited flexibility.?[mechanical stimulation卪echanoreception from muscle spindles]
Subjects in both groups exercised three times per week for 8 weeks.
The aerobic exercise program comprised walking on treadmill, initially for 20 min and increasing up to 30 min per patient tolerance. Exercise intensity was adjusted to generate heart rates equivalent to 60?0% of age-adjusted maximum heart rates (220 minus age in years).
Patients in the SE group received a supervised, progressive physical training program, with muscle strengthening of the upper and lower limb muscles and trunk muscles, initially with 4? repetitions and progressing to 12 repetitions gradually.
Patients began with resistance levels they could do easily, and weight was increased gradually according to patient抯 tolerance.
Outcome measures were the intensity of fibromyalgia-related symptoms (pain, fatigue, sleep disturbance), tender point count, cardiovascular fitness, psychological status, and quality of life.
Pain intensity was measured with visual analog scale (VAS).
揅ardiovascular fitness was assessed by 6-min walk test, which is a reliable and valid measure in fibromyalgia patients.?Subjects were instructed to walk as far as they could at a fast, comfortable pace in 6 min. The distance walked in 6 min was recorded.
The SF-36 was used to evaluate quality of life. The SF-36 is a generic measure of quality of life addressing eight health concepts: physical functioning, role physical, bodily pain, vitality, role emotional, social functioning, mental health, and general health. Scores for each dimension range from 0 (poor health) to 100 (good health).
None of the patients had a habit of regular physical activity before participating in the study.
There were similar significant improvements in both groups regarding pain, sleep, fatigue, tender point count, and 6-min walk distance after treatment. HAD scale-depression scores improved significantly in both groups as well.
DISCUSSION
揙ur study demonstrated that pain, sleep, fatigue, tender point counts, 6-min walk distances, depression, and quality of life improved to a similar degree after SE and AE in patients with fibromyalgia syndrome.?
揘o patient experienced musculoskeletal injury or exacerbation of fibromyalgia-related symptoms during the intervention.?
The magnitude of change was generally greater in the strengthening group v. the aerobic group in other similar investigations.
In this study, there was significant improvements in fibromyalgia symptoms and tender point counts in both groups. [IMPORTANT]
揝ix-minute walk distance increased 41 m in the AE group and 77 m in the SE group.?br>
In this study, the improvement in 6-min walk distance was greater in the SE group than the AE group. 揟his finding suggests that muscle strengthening may be more important than aerobic training in improving fitness in fibromyalgia patients.?br>
揑n healthy individuals and individuals with psychiatric disease, exercise is known to improve depression and anxiety.?br>
揃oth AE and resistance training have been shown to reduce depressive symptoms.?br>
揑n conclusion, aerobic exercise and strengthening exercise were similarly effective at improving symptoms, tender point count, fitness, psychological status, and quality of life in fibromyalgia patients.?
KEY POINTS FROM SUNCOAST HEALTHCARE PROFESSIONALS
1) 揊ibromyalgia is a chronic painful condition characterized by widespread pain, pain at specific tender points, sleep disturbance, and fatigue.?br>
2) Fibromyalgia is more common in females than males.
3) 揟he majority of patients with FM are known to be aerobically unfit and have poor muscle strength and limited flexibility.?
4) 揑t is widely accepted that exercise is beneficial for patients with fibromyalgia.?br>
5) The aerobic exercise program comprised walking on treadmill, initially for 20 min and increasing up to 30 min as the patient tolerated. Exercise intensity was adjusted to generate heart rates equivalent to 60?0% of age-adjusted maximum heart rates (220 minus age in years).
6) Patients in the SE group received a supervised, progressive physical training program, with muscle strengthening of the upper and lower limb muscles and trunk muscles, initially with 4? repetitions and progressing to 12 repetitions gradually. Patients began with resistance levels they could do easily, and weight was increased gradually according to patient抯 tolerance.
7) Outcome measures were the intensity of fibromyalgia-related symptoms (pain, fatigue, sleep disturbance), tender point count, cardiovascular fitness, psychological status, and quality of life.
8) Pain intensity was measured with visual analog scale (VAS).
9) 揅ardiovascular fitness was assessed by 6-min walk test, which is a reliable and valid measure in fibromyalgia patients.?
10) The SF-36 was used to evaluate quality of life. The SF-36 is a generic measure of quality of life addressing eight health concepts: physical functioning, role physical, bodily pain, vitality, role emotional, social functioning, mental health, and general health. Scores for each dimension range from 0 (poor health) to 100 (good health).
11) In this study, pain, sleep, fatigue, tender point counts, 6-min walk distances, depression, and quality of life improved to a similar degree after strengthening and aerobic exercise in patients with fibromyalgia syndrome.
12) No patient experienced musculoskeletal injury or exacerbation of fibromyalgia-related symptoms during the intervention. [IMPORTANT]
13) The magnitude of change was generally greater in the strengthening group v. the aerobic group.
14) 揗uscle strengthening may be more important than aerobic training in improving fitness in fibromyalgia patients.?br>
15) 揑n healthy individuals and individuals with psychiatric disease, exercise is known to improve depression and anxiety.?br>
16) 揃oth aerobic exercise and resistance training have been shown to reduce depressive symptoms.?br>
17) 揑n conclusion, aerobic exercise and strengthening exercise were similarly effective at improving symptoms, tender point count, fitness, psychological status, and quality of life in fibromyalgia patients.?
---------- FOLLOW-UP ----------
QUESTION: Where ARE you? I want you to be my health care professional! =) Thanks so much for all of the information. I can't tell you how much I appreciated the lengthy and knowledgeable answer. It's really going to help me! - Angel
P.S. My chiropractor did take x-rays and did a mobility test somewhat. Not sure about everything else. He is aware of what I am experiencing and believes the treatment was too aggressive. I've discontinued the treatment. I intend to follow ALL of your advice, exercise and take my vitamins. (I never heard of malate. I've got some homework to do!) If I have not recovered completely from the burning spine and neck pain within a week or so I will make sure I get an MRI. I must say there is a slight improvement with lots of bed rest this weekend, as the burning is more confined to the upper body now. THANKS AGAIN, Dr. Leatherman!
AnswerDear Angel,
Thanks for the kind words. I understand your enthusiasm as it is often hard to get a straight answer from doctors of all disciplines, and often answers are not generated from clinical research. Glad to feel that you are starting to feel better and that you have been in contact with your chiropractor...hopefully you won't need the MRI.
If you wish to try the Complete FM product that I mentioned in the research, you have to get it from a health care professional as they do not sell to the public. So if your chiropractor and medical doctor do not carry Nutriwest products, I would be happy to order it for you... just call my office and Kelly the office manager can take care of it for you.
By the way, I practice in the panhandle of Florida (Fort Walton Beach), so if you come for vacation (the water is warm and beautiful), look us up. And if you need any further assistance, please feel free to write back. Good luck!!
Respectfully,
Dr. J. Shawn Leatherman
www.suncoasthealthcare.net