Traumatic dislocations of the hip are an orthopedic emergency. Although the diagnosis of the common posterior hip dislocation may often be straightforward, the emergent diagnosis and reduction of the dislocation, especially in light of multiply traumatically injured trauma patient, can be challenging. High-energy blunt force trauma is the most common cause, although prosthetic hip joints may dislocate with much less force. Multiple studies have shown that timely reduction plays a significant role in reducing later complications and associated comorbidity. As a result, the routine screening for this injury has been adopted in the evaluation of trauma patients.[1, 2, 3, 4, 5, 6, 7, 8, 9, 10]
Congenital dislocation of the hip also occurs and is termed developmental dysplasia of the hip (DDH). The annual incidence of DDH is approximately 2-4 cases per 1000 births; approximately 80-85% of the affected individuals are girls. Routine screening for DDH includes the Barlow and Ortolani tests, with further tests such as ultrasound for cases prompting concern. The focus of this article is on traumatic dislocations.
NextThe hip is a modified ball-socket joint. The femoral head is situated deep within the acetabular socket, which is further enhanced by a cartilaginous labrum. The hip is also bolstered by a fibrous joint capsule, the ischiofemoral ligament, and many strong muscles of the upper thigh and gluteal region. Because of this anatomic configuration, the hip is stable, as in the image below.
 A normal anteroposterior (AP) pelvis radiograph.
A normal anteroposterior (AP) pelvis radiograph.
Subsequently, a large force is required to dislocate the joint. Because a high force mechanism is required, other life-threatening injuries and fractures are common.
Motor vehicle crashes (MVC) account for two thirds of traumatic hip dislocations, but falls from height are also a significant cause, whereas sport injuries are a less common cause.
Hip dislocations can be divided into simple and complex, with the later having associated fractures. The relationship of the femoral head to the acetabulum is used to classify the dislocation. The three main patterns are posterior, anterior, and central.
Posterior dislocations comprise approximately 80-90% of hip dislocations caused by MVCs. The femoral head is situated posterior to the acetabulum. During a MVC, force is transmitted to the flexed hip in one of two ways. During rapid deceleration, the knees strike the dashboard and transmit the force through the femur to the hip. If the leg is extended and the knee is locked, force can be transmitted from the floorboard though the entire lower and upper leg to the hip joint. A posterior dislocation is shown in the image below.
 Right posterior hip dislocation in a young woman following a high-speed motor vehicle collision (MVC).
Right posterior hip dislocation in a young woman following a high-speed motor vehicle collision (MVC).
The femoral head is situated anterior to the acetabulum. An anterior dislocation is most commonly caused by a hyperextension force against an abducted leg that levers the femoral head out of the acetabulum. Less commonly, an anterior force against the posterior femoral neck or head can produce this dislocation pattern.
Anterior hip dislocations have been reported to account for approximately 5-10% of all hip dislocations. Of all anterior hip dislocations, inferior or obturator dislocations have been found to be more common, constituting approximately 70% of all anterior dislocations. Risk factors for closed reductions of anterior hip dislocations include preexisting osteopenia on plain films, age greater than 65 years, and radiographic femoral head impingement on the surrounding bony pelvis. In one study, closed reduction of both anterior and posterior hip dislocations were noted to be urgent and should occur within 6 hours after the time of dislocation.[7]
A central dislocation is always a fracture-dislocation. As shown in the image below, the femoral head lies medial to a fractured acetabulum. This is caused by a lateral force against an adducted femur as commonly seen in side impact MVCs. A central fracture-dislocation is shown in the image below.
 Fracture-dislocation of the right hip. The bony fragments are likely part of the acetabulum.
Fracture-dislocation of the right hip. The bony fragments are likely part of the acetabulum.
United States
Posterior hip dislocations are more common than anterior ones and account for almost 90% of hip dislocations. The frequency has decreased with the increased use of seat belts and air bags. Anterior dislocations and central fracture-dislocations account for less than 10% of hip dislocations.
Most studies have found the incidence of dislocation after total hip arthroplasty (THA) to be approximately 2-5%, with the almost three fourths of those dislocations occurring in the first 6 weeks after surgery.[11]
International
All claims data from a large sample of a comprehensive health database in Taiwan illustrated several points regarding the epidemiology of hip dislocation that may be generally informative:[12]
Additionally, a recent report from a developing country indicate that the incidence of traumatic hip dislocations may be increasing due to a greater number of high-speed motor vehicle accidents,[13] a phenomenon that may be repeated globally as larger populations have access to motor vehicles.
Hip dislocation is a marker for a high force mechanism. Most mortality is the result of associated injuries. Life-threatening injuries to the pelvis, abdomen, chest, and head should be specifically sought out.
Long-term disability after hip dislocations is a significant risk. Up to 50% of patients will have limited use or chronic pain as a result of hip dislocation. Prognosis becomes worse with delayed diagnosis and management. Complications include deep venous thrombosis (DVT), sciatic nerve injury, avascular necrosis (AVN), vascular injury, recurrent dislocation, arthritis, and chronic pain.
The local venous injury and prolonged immobilization associated with hip dislocations lead to a significant incidence of deep venous thrombosis (DVT) and potentially lethal pulmonary embolus in affected patients. If no contraindications exist, patients should receive DVT prophylaxis as part of the hospital and rehabilitation treatment.
Sciatic nerve injury is common, up to 19% in one study. The femoral head or bony fragments can stretch or tear the nerve as it passes posterior. The neurapraxia is generally transient or minor. A full recovery or recovery with only minor neurological findings can be expected for most patients. Performing and documenting a brief neurological examination before and after relocation is imperative.
Avascular necrosis of the femoral head occurs in 2-17% of patients. This can occur with pure dislocations but is more common with fracture-dislocations of the femoral head. Numerous studies suggest that the risk of AVN rises proportional to the time to relocation. The longer it takes to relocate a hip, the higher the risk of AVN. Early relocation of a hip can make the difference between a healthy joint and a chronically disabled joint.
Vascular compromise is a rare. With anterior dislocations, the femoral artery is at risk. Pulses and perfusion should be checked and documented before and after reduction. If a patient has vascular compromise, reducing the hip should not be delayed. If a patient has a persistent or new-onset perfusion deficit, an open reduction and consultation with a vascular surgeon may be indicated.
Recurrent hip dislocation is uncommon compared to recurrent shoulder dislocation. Risk factors for recurrent dislocation are large capsular defects, intra-articular fragments, or a prosthetic hip.
Posttraumatic arthritis is the most frequent long-term complication following hip dislocation. It occurs in up to 16% of affected individuals and is often associated with life-long gait disturbances and chronic pain. If an associated acetabular fracture is present, the incidence of traumatic arthritis is as high as 80%.
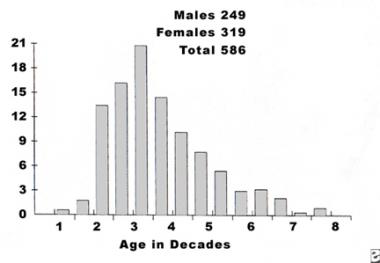
Hip dislocations are more common in young males than in others because these injuries are associated with risk-taking behavior.
In a study of sports-related hip injuries on the basis of sex and age in young athletes, the main diagnoses for males were labral tear (23.1%), avulsion fracture (11.5%), slipped capital femoral epiphysis (11.5%), dislocation (7.7%), and tendonitis (7.7%). The main diagnoses for females were labral tear (59.0%), tendonitis (14.8%), snapping hip syndrome (6.6%), strain (4.9%), and bursitis (4.9%). The proportion of hip injuries in the female athletes showed a significantly greater increase with advancing age than that seen in males.[14]
Hip dislocations resulting from traumatic injuries (especially MVCs) are more common in those younger than 35 years than in older people. Hip dislocations resulting from falls are more common in those older than 65 years than in younger people.
The prognosis of the patient with a hip dislocation varies with the type of dislocation, with the associated fractures of the femoral head or acetabulum, and the presence of other injuries. Overall, good-to-excellent results are obtained in 50-93% of patients.
The principal determinants of a poor prognosis are as follows:
For excellent patient education resources, see eMedicineHealth's patient education article Total Hip Replacement.
Clinical Presentation
Copyright © www.orthopaedics.win Bone Health All Rights Reserved