Osteoblastoma is a rare primary neoplasm of bone, categorized as a benign bone tumor that is closely related to osteoid osteoma. It is a bone-forming lesion that may be found within the cortex, medullary canal, or periosteal tissues; multicentric foci within a single bone have also been described. There is a slight predominance of metaphyseal over diaphyseal locations.[1] Osteoblastoma differs from osteoid osteoma in its ability to grow larger than 2.0 cm in diameter and its aggressive behavior in bone.[2, 3, 4, 5, 6, 7, 8]
In his original description of osteoblastoma, Lichtenstein termed the lesion an "osteogenic fibroma of bone."[9, 10] In 1954, Dahlin and Johnson reported 11 aggressive but benign tumors that appeared to originate within bone and were frequently difficult for the inexperienced pathologist to differentiate from malignancy.[11] They chose to call the tumor a giant osteoid osteoma for its histologic similarity to osteoid osteoma. The current and accepted name, osteoblastoma, was coined by Lichtenstein and Jaffe in their independent and more detailed reports of this neoplasm.[9, 12]
The clinical course of osteoblastoma often makes diagnosis difficult. The tumor may have a slow indolent course or display characteristics that are confused with malignancy, especially if it has an aneurysmal bone cyst component. Other diagnoses that share similar clinical, radiographic, and histologic features with conventional osteoblastoma include osteoid osteoma. Osteoblastomas may also have features that mimic malignant tumors, which often make it difficult for inexperienced surgical oncologists and pathologists to diagnose. Osteoblastoma is about 20 times less common than osteosarcoma is.[2, 13, 14, 15, 16, 17]
NextOsteoblastoma commonly affects the vertebral column, with approximately 30% of these lesions arising within the posterior elements of the spine. The vertebral body has been reported as the primary origin of these neoplasms in some reports, but these locations may be due to the failure to clearly identify the epicenter of the neoplasms (see the images below). Equally common locations (30%) are the long bones of the appendicular skeleton, typically the femur and the tibia, as is the case with all benign and malignant bony neoplasms.
 Standard radiograph of an osteoblastoma with a secondary aneurysmal bone cyst of the lumbar spine.
Standard radiograph of an osteoblastoma with a secondary aneurysmal bone cyst of the lumbar spine.
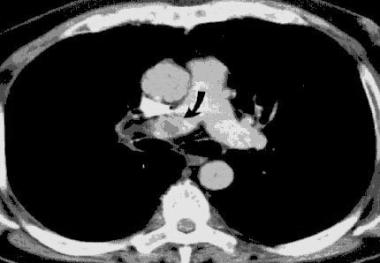
 (Click image to enlarge.) Osteoblastoma with a secondary aneurysmal bone cyst. CT findings are nonspecific but help demonstrate the extent of lesion arising in the vertebral column.
(Click image to enlarge.) Osteoblastoma with a secondary aneurysmal bone cyst. CT findings are nonspecific but help demonstrate the extent of lesion arising in the vertebral column.
Other documented locations of osteoblastoma include the pelvic bones, the small bones of the hands and feet, the skull/facial bones, the clavicle, the scapula, and the ribs. Osteoblastoma also arises in the talus more frequently than other benign tumors do (see the image below).[18, 19, 20, 21, 22]
 Oblique and lateral radiographs of the ankle reveal a lucent lesion within the talus.
Oblique and lateral radiographs of the ankle reveal a lucent lesion within the talus.
Associated aneurysmal bone cysts (see the image below) may be seen with as many as 10% of osteoblastomas, imparting to these lesions much more aggressive and alarming characteristics.
Standard radiograph of an osteoblastoma with a secondary aneurysmal bone cyst of the lumbar spine.
Regardless of where osteoblastomas originate within the musculoskeletal system, they are composed of numerous osteoblasts that produce osteoid and woven bone. When the primary site is within cortical bone, expansion is often present. However, the outer rim of the tumor is always covered by periosteum and a thin rim of reactive bone. In the largest series reported, the size of osteoblastomas ranged from 1 to 11 cm, with a mean of 3.2 cm.[23]
As opposed to more their benign counterparts, aggressive osteoblastomas display aggressive destruction of the adjacent host bone cortex and extends into surrounding soft tissues. This characteristic is thought to be due to a coexisting aneurysmal bone cyst component.
The exact etiology of osteoblastoma is unknown.
In the United States, osteoblastoma accounts for approximately 1% of all primary bone tumors. The mean age at presentation in the largest series studied was 20.4 years, with a range of 6 months to 75 years.[23] The male-to-female patient ratio is 2:1.
Osteoblastoma has a reported recurrence rate of approximately 10-20%. Tumor relapse is associated with inadequate resection of the primary lesion. In some areas (eg, the spine), it might not always be possible to remove the entire lesion.
For stage 2 osteoblastomas (see Workup, Staging), however, the overall recurrence rate after extensive intralesional excision is close to 0%. The recurrence rate after excision through the reactive zone of the bone (marginal excision) is much higher. For an osteoblastoma associated with an aneurysmal bone cyst, the recurrence rate after wide excision in surgically accessible sites is reported as low, but no large-scale studies exist to define what "low" means. The recurrence rate after intralesional excision is higher at any site, as expected.
Clinical Presentation
Copyright © www.orthopaedics.win Bone Health All Rights Reserved