Patella fractures account for approximately 1% of all skeletal injuries. They become problematic if the extensor mechanism of the knee is nonfunctional, articular congruity is lost, or stiffness of the knee joint ensues. To avoid these problems, the surgeon must achieve anatomic restoration of the joint and must allow early motion.
In the 1800s, treatment of patella fractures was controversial. Owing to a lack of adequate fixation techniques, surgical experience, and imaging, treatment most often consisted of extension splinting. This led to poor results because of intra-articular incongruity, nonunion, and poor motion.
Initial attempts at operative stabilization of these fractures yielded satisfactory repair rates lower than 50%. Treatment then progressed to excision of fractured patellar fragments or of the entire patella. Despite encouraging early results, long-term follow-up revealed degenerative changes in the femoral condyles and decreased quadriceps power.[1, 2, 3, 4, 5, 6, 7]
With the introduction of the AO group (Arbeitsgemeinschaft für Osteosynthese, or Association for the Study of Osteosynthesis) in the 1950s, a new technique for fixation of these fractures was developed. The concept of the anterior tension band technique was introduced. This allowed stable fixation, early motion, and improved rates of bony union.
NextThe patella is the largest sesamoid bone in the body. It is contained within the extensor mechanism, consisting of the quadriceps tendon proximally and the patellar ligament distally. At this location, it serves to increase the extensor moment by nearly 30%. The patella is covered at its proximal aspect by thick cartilage. Owing to its relatively small size, the patellofemoral joint is exposed to the highest contact stress of any weightbearing joint. Therefore, any aberration in its anatomy or alignment may lead to symptomatic degenerative changes.
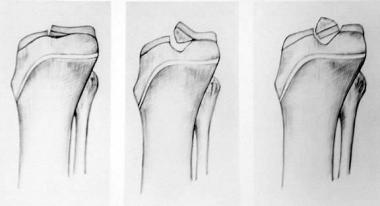
The subcutaneous location of the patella makes it prone to injury. Fractures occur as a result of a compressive force (as occurs with a direct blow), a sudden tensile force (as occurs with hyperflexion of the knee), or a combination of these. Various fracture patterns result, depending on the mechanism of injury. The most common patterns are often described as stellate or transverse; less common patterns include vertical, marginal, osteochondral, and sleeve fractures.
Sleeve fractures are seen exclusively in the pediatric population.[8] On radiographs, sleeve fractures are represented by a small bony avulsion fracture. However, they are actually larger than they appear on radiographs because they are surrounded by a significant portion of articular cartilage.
A direct blow to the patella most often results in a stellate fracture. The compressive forces applied to the patella result in a comminuted pattern. The energy of the blow is absorbed by the fracture and may cause damage to the articular cartilage of both the patella and the femoral condyles. Free osteochondral lesions, therefore, must be excluded. About 65% of these fractures do not involve the extensor retinaculum. If the extensor mechanism has not been disrupted and if intra-articular stepoff is less than 2 mm, the fracture may be treated nonoperatively.
Another mechanism of injury to the patella is a tensile force, as is sustained with hyperflexion of the knee with an eccentric contraction of the quadriceps. Approximately 35% of these are nondisplaced fractures with an intact retinaculum. This type of fracture, with less than 2 mm of intra-articular stepoff, can be treated with a nonoperative modality.
A combination of these two mechanisms can lead to a variety of other fracture patterns. A displaced transverse fracture can have comminution if a blow to the knee occurs after the tensile force. For instance, a hyperflexion moment to the knee resulting in a transverse fracture pattern can be followed by a fall onto the knee, which causes comminution.
The prognosis depends primarily on the quality of articular restoration.[9] Any intra-articular incongruities lead to posttraumatic arthritis. To a certain extent, the prognosis also depends on the amount of chondral damage sustained at the time of injury. Some of these changes are irreversible; anatomic restoration of the joint minimizes the long-term degenerative changes. Functional outcome depends on the ability to achieve early, pain-free, stable range of motion. If arthrofibrosis develops, it may require manipulation with the patient under anesthesia or arthroscopic release of adhesions.
Rabalais et al compared two tension-band techniques, with stainless-steel wire and ultra-high-molecular-weight polyethylene cable, in transverse patella fractures in eight cadaver knees.[10] Fixation consisted of figure-eight and parallel wire configurations, along with Kirschner wires (K-wires) and polyethylene cable. The parallel wire configuration showed better results than the figure-eight construct in monotonic and cyclic loading models, and the ultra-high-molecular-weight polyethylene cable and the 18-gauge steel wire performed similarly.
El-Sayed and Ragab reported on arthroscopic-assisted reduction and fixation of displaced transverse fractures of the patella in 14 patients with displaced transverse fractures of the patella.[11] Patients were treated by means of arthroscopic-assisted closed reduction of the fracture with percutaneous screw fixation. Patella fractures were found to unite in a mean of 7 weeks. All 14 patients regained full extension of the knee, and full range of motion was achieved in 12 patients, with two patients experiencing a 10º loss of flexion.
Wright et al performed materials testing on No. 5 FiberWire suture and 18-gauge stainless-steel wire tension by using them both for band fixation on a transverse patellar fracture model and performing three-point bending tests.[12] The investigators found that FiberWire maintained its initial stiffness until failure and that during three-point bend testing, double-strand FiberWire had a higher failure load than stainless-steel wire when the suture was tied and locked under tension created by a modified Wagoner hitch.
Dargel et al compared interfragmentary compression with tension band wiring.[13] They concluded that fragment fixation is an acceptable technique for treating osteosynthesis of a transverse patella fracture.
Muzaffar et al successfully treated minimally displaced two-part patellar fractures with percutaneous K-wire fixation and compression that was subsequently augmented with a cast.[14]
In a retrospective study of 72 patients with transverse patella fractures treated with either a modified tension band (n=37) or a titanium cannulated lag screw (n=35), Wang et al found that the parallel titanium cannulated lag screw technique yielded better results; accordingly, they recommended that this technique be considered as an alternative method for treating transverse patella fractures.[15]
Clinical Presentation
Copyright © www.orthopaedics.win Bone Health All Rights Reserved