Sprengel deformity is a complex anomaly that is associated with malposition and dysplasia of the scapula.[1, 2, 3, 4, 5] This condition also involves regional muscle hypoplasia or atrophy, which causes disfigurement and limitation of shoulder movement. Sprengel deformity is the most common congenital malformation of the shoulder girdle.[6] The male-to-female ratio is 3:1.
In 1863, Eulenberg first described what later became known as Sprengel deformity.[7] Two decades later, Willet and Walsham reported two cases with anatomic descriptions of this clinical entity.[8] Sprengel then described four cases of upward displacement of the scapula in 1891.[9] Kolliker, who also described four cases in 1891, gave the condition its eponym, Sprengel deformity.[10] Multiple case reports and surgical techniques followed in the literature for Sprengel deformity (also referred to as congenital elevation of the scapula).
For patient education resources, see Spina Bifida and Scoliosis.
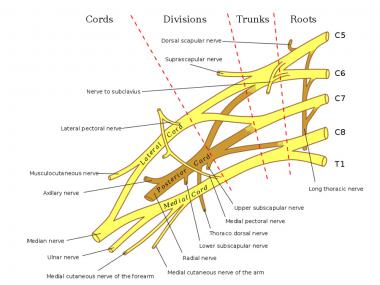
NextSome vital structures are at risk during the extensive dissection that is required as part of the relocation procedure. These structures include the following[11] :
The dorsal scapular nerve courses close to the superomedial border of the scapula in the plane between the rhomboid and the erector spinae. The dorsal scapular nerve remains anterior to the serratus anterior and the subscapular muscles.
There exists a risk of injuring the dorsal scapular nerve during dissection of the periscapular muscles at the superomedial angle of the scapula, and when the trapezius and rhomboid muscles are reflected off as a single unit from the spine in the Woodward procedure (see Treatment). Therefore, staying subperiosteal during the process of freeing the periscapular muscles is essential, especially at the superomedial angle of the scapula.
The spinal accessory nerve is located between the trapezius and rhomboid muscles and therefore is theoreticallyat risk; however, because this nerve is sandwiched between the two muscles, it is rarely ever injured when these muscles operate as a unit.
The suprascapular nerve runs in the suprascapular notch of the scapula and may be injured if the dissection is carried too far laterally when the superior portion of the scapula is resected. By staying at least 1 cm medial to the notch, injury to the nerve during the procedure can be avoided.
Despite the work of Engel (Bleb theory), Oxnard, and Ogden et al, no satisfactory explanation exists regarding the pathogenesis of the Sprengel deformity.[3, 12, 13, 14]
Grossly, the scapula is dysplastic and is located higher than normal in the neck or upper thoracic region. This bone is smaller than normal in the vertical plane and appears larger horizontally. The inferior angle is rotated medially, causing the glenoid to face inferiorly.
An inverse correlation exists between the superior displacement and rotation of the scapula; with a higher scapula, the rotation is decreased. Convexity of the upper (supraspinous) portion of the scapula is increased and curvature of the clavicular shaft is decreased, forming a narrower scapuloclavicular space, which may contribute to brachial plexus compression postoperatively.
An omovertebral connection, which may be fibrous, cartilaginous, or bony, may exist in about one third of cases.[1, 6] This connection attaches the superomedial angle of the scapula to the spinous process, lamina, or transverse process of the cervical vertebrae and may be the primary cause of restricted shoulder motion in patients with a Sprengel deformity.[15]
The omovertebral connection is usually unilateral, is always associated with a fixed, elevated scapula, and has a major role in determining the shape and the malpositioning of the scapula.[16, 17] According to Willet and Walsham, the omovertebral bar is homologous to the suprascapular bone in lower vertebrates.[8]
The spinoscapular muscles may be fibrotic and contracted; the trapezius is the muscle most commonly affected.
The condition is sporadic. Rarely, it may run in families (autosomal dominant pattern of inheritance).[18, 19]
The scapula is a cervical appendage that normally differentiates opposite the fourth, fifth, and sixth cervical vertebrae at about 5 weeks' gestation.[20] This structure normally descends to the thorax by the end of the third month of intrauterine life; any impediment to its descent results in a hypoplastic, elevated scapula, known as the Sprengel deformity.
Congenital elevation of the scapula is caused by an interruption in the normal caudad migration of the scapula. This produces both cosmetic and functional impairment and probably occurs between weeks 9 and 12 of gestation.
An arrest in the development of bone, cartilage, and muscle also occurs. The trapezius, rhomboid, or levator scapulae may be absent, hypoplastic, or contain multiple fibrous adhesions. The serratus anterior may be weak, leading to winging of the scapula. Other muscles, such as the pectoralis major, latissimus dorsi, or the sternocleidomastoid, may be hypoplastic and similarly involved.
Associated malformations are almost always present with a Sprengel deformity. These can include anomalies in the cervicothoracic vertebrae or the thoracic rib cage. The most common anomalies are absent or fused ribs, chest-wall asymmetry, Klippel-Feil syndrome, cervical ribs, congenital scoliosis, and cervical spina bifida. When scoliosis is present, the most common curves are in the cervicothoracic or upper thoracic region. A relationship between a Sprengel deformity and diastematomyelia has also been shown.
Another anomaly, seen in about one third of these patients, is the omovertebral bone. This is a rhomboid- or trapezoid-shaped structure of cartilage or bone that usually lies in a strong fascial sheath, which extends from the superomedial border of the scapula to the spinous processes, lamina, or transverse processes of the cervical spine (most commonly C4-7). A well-developed joint can form between this bone and the scapula; the bone can also be a solid osseous bridge. The omovertebral bone is best visualized on a lateral or oblique radiograph of the cervical spine.
Prognostic factors include the following:
Copyright © www.orthopaedics.win Bone Health All Rights Reserved