Fractures of the humeral shaft account for approximately 3% of all fractures.[1, 2] Traditionally, humeral shaft fractures have been described according to the following features[2] :
This article focuses on midshaft humerus fractures.
No classification scheme for humeral shaft fractures has gained universal acceptance. The Arbeitsgemeinschaft für Osteosynthesefragen–Association for the Study of Internal Fixation (AO-ASIF) classification is based on the amount of comminution, as follows:
Although most fractures of the humeral shaft are inherently unstable, nonoperative treatment remains the standard.[3] For operative candidates, the role of surgery, as well as which type of surgery is appropriate, is dependent on the patient and the fracture characteristics.[4, 5]
For patient education resources, see the First Aid and Injuries Center, as well as Broken Arm.
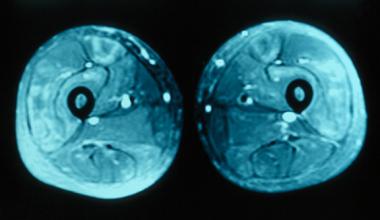
NextThe humeral shaft is the area extending from the upper border of the pectoralis major tendon to the supracondylar ridge. The proximal half is almost cylindrical, whereas distally, the anteroposterior diameter narrows into a prismatic shape. The posterior surface (between the medial and lateral borders) is the largest. The radial sulcus, which contains the radial nerve and, at its midpoint, the nutrient foramen, crosses the posterior middle third of the humerus.
The large muscles that surround the humerus prevent direct palpation. The arm is divided into anterior and posterior compartments by two intermuscular septa: medial and lateral.[6] The anterior compartment contains the following:
The posterior compartment contains the following:
Each method of humeral shaft fracture treatment is associated with a union rate of higher than 90%. Each fracture must be considered separately and treated accordingly.[7]
Connolly et al assessed the outcome of immediate open reduction and internal fixation (ORIF) in 46 patients with open humeral diaphyseal fractures.[8] All fractures united primarily in satisfactory angulation of less than 5º in coronal and sagittal planes. In 40 patients, mean time to union was 18.4 weeks; in six, union was delayed (mean time to union, 42.5 weeks). No patient required subsequent surgery to obtain union. Complications were rare (including amputation in three patients and dysesthesia in one), with no deep infections, nonunions, or iatrogenic nerve injuries. Two implants were removed because of discomfort.
Heineman et al conducted a meta-analysis of four trials comparing treatment of humeral shaft fractures with different implants (plates and nails).[9] After calculating the data from the four trials (203 patients), they did not find any statistically significant differences between plates and nails with respect to complications, nonunion, infection, nerve palsy, or reoperation.
In a retrospective study, Pretell et al reported that 17 of 19 patients with fractures of the humeral shaft treated with anterograde locked intramedullary nailing were satisfied with the results.[10] The mean duration of hospitalization after surgery was 4.3 days; there were no complications related to the implants; there were no operative complications; and the average operation time was 48 minutes. The consolidation rate was 80%.
Clinical Presentation
Copyright © www.orthopaedics.win Bone Health All Rights Reserved