Background
Cervical disc protusions, if they compress the nerves in the neck typically cause arm pain. There are a number of operative ways that this can be managed but, if suitable, a posterior cervical foraminotomy is a vastly under-rated operation which avoids some of the shortcomings of other disc operations and yet still has an excellent outcome in terms of symptom relief, in a minimally invasive fashion.
The typical patient presents with pain down one arm which may radiate to the hand. Cervical disc problems are exceedingly common and it is important to realise that in the vast majority of cases non-operative management works very well. Most patients settle within 6-12 weeks after the onset of symptoms. The pathophysiology of why a patient gets symptoms is disc protusion is complex, as not all disc patients get pain.
A posterior cervical foraminotomy is a minimally-invasive procedure designed to enlarge to space through which the nerve root exits from the spinal cord (the so-called neural foramen) and at the same time try to remove any piece of disc which is pushing on the nerve. Interestingly, sometimes the foraminotomy alone can alleviate symptoms without a discectomy being needed. The whole disc is not removed, just the fragment pressing the nerve root. A fusion is not performed and most patients typically do not require a neck collar after the surgery.
A disc protusion per se may not cause symptoms. If the anulus is acutely torn, neck pain may result, but the management is usually not operative. If the disc pushes on a nerve, as shown in the previous scans, then symptoms down one or occasionally both arms may result. The symptoms can include pain, numbness, ?pins and needles?, and weakness.
Anatomy
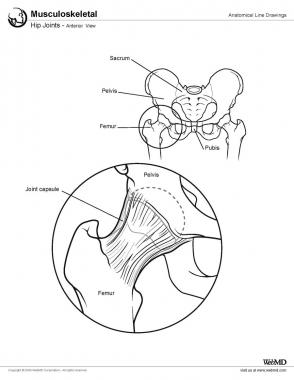
The anatomy of a typical intervertebral disc as shown below:
(Below): The intervertebral disc lies in front of the spinal nerves and is situated between the vertebral bodies. It carries 80% of the load transmitted through the neck and is the shock absorber for the spine. The lowermost discs of the neck (C56 and C67) are most prone to wear and tear and potential rupture.
Note that there is an outer shell, called the anulus fibrosis and an inner core called the nucleus pulposus. The anulus is the consistency of a pencil eraser, whereas the nucleus is gel-like and, as we get older, dehydrates and becomes like crabmeat. The discs act as shock absorbers and flexing the spine loads the disc.
A tear in the outer anulus can consequently cause severe neck pain. Once an anular tear occurs, it may heal, or it may allow nucleus to come out of the centre of the disc, into the spinal canal, where it may compress nerves. This is usually called one of a number of terms, including disc prolapse, ruptured disc, slipped disc, and extruded disc. All these terms essentially mean the same thing. Once nerves are compressed, surgery may be complicated. It is important to know that the prolapsed disc cannot be pushed back into place and nothing but time will heal the anular tear. Thus, in general, any surgery using this approach is aimed at improving the arm pain, not the neck pain.
Reason For Operation
Cervical disc protrusions are not usually operated upon early, but there are some clear situations when a surgeon may recommend early surgery. If there is evidence of severe weakness, early surgery may be offered. If the pain in the arm is so severe that narcotic analgesia is not controlling the pain, early surgery may again be an option. Finally, if there is a suggestion of spinal cord compression, and myelopathy, early surgery is advocated. A posterior cervical foraminotomy is not the operation of choice if a disc protusion is causing myelopathy as this typically indicates that the compression of the spinal cord is from disc material in front of the cord. Consequently, a posterior approach such as for a cervical foraminotomy is not suited for spinal cord compression and myelopathy.
If a patient has pain, but it is not too severe, then typically conservative management is initiated. It must be remembered that the vast proportion of patients will settle with time and as long as improvements are noted at 6 weeks, there is minimal or no weakness, and the pain is not excruciating and is liveable with oral analgesia, then waiting and continuing with conservative therapy is a good option.
If weakness occurs and is not improving, surgery is usually offered. Similarly, if symptoms are not improving at 6 weeks then surgery is an option.
In most cases, when managing just arm pain, surgery is a treatment option that speeds up the rate of recovery, remembering that most cases will get better by themselves. Again, specific recommendations are tailored to the patient. In the vast number of cases, the goal is control of pain, and any intervention that achieves this and is less invasive than surgery is a reasonable option.
Copyright © www.orthopaedics.win Bone Health All Rights Reserved