Question Hi, I had a back injury from repetitive lifting and twisting at work back in early Feb. I had some back pain before the injury but it always went away though a few weeks prior I did have a feeling that something was loose in my left hamstring like a rubber band snapped? it's hard to explain it wasn't very painful just a weird feeling. The day of the accident I felt a sharp shock like feeling that went down my left leg and made my foot tingly. Long story short it's now been 5 months and I still have a numb feeling on top of my foot and lower shin the awful burning lower back pain has diminished alot but the numbness remains? and does effect walking. No jogging running etc. What puzzles me
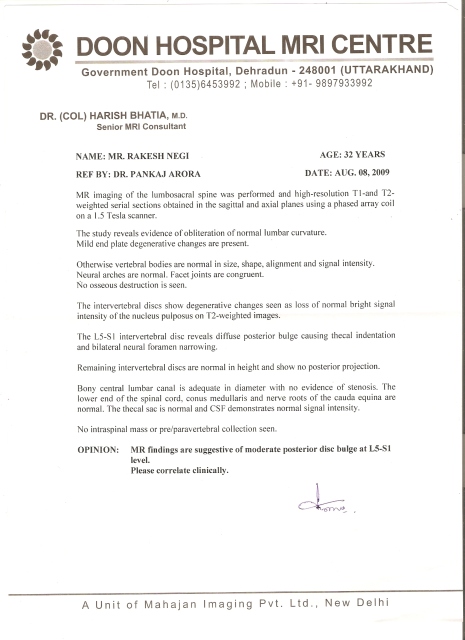
is that the MRI showed no significant place where the nerve was being irritated. I also had an EMG that showed normal signal everywhere except behind my knee? an MRI of that was negative but the radiologist noticed some loss of muscle signal by the Peraneal nerve? The doctor wants another MRI with contrast not sure if it will be approved since it's an LNI deal. I am doing regular physical therapy and it has definitely helped the back pain alot. I'm just down because the numbness hasn't decreased. Is it possible to have that
symptom from a lower back injury but not show up on an MRI as disc related? very frustrating thank you
AnswerHi Tim,
This shouldn't be frustrating at all, an MRI of your entire body won't show what you have. I strongly suspect a common injury of the peroneal nerve. They just don't know how to visualize it or reproduce it. I have successfully treated dozens of these cases. Try walking on your heals, I doubt it will be easy on the left side. We call this "foot drop". From what you explained, it sounds like a classic case of peroneal nerve entrapment and/or blunt injury or inflammation at the proximal head of the fibula.
Just below the outside lateral side of the left knee, the nerve passes over the head of the fibula, making it very vulnerable to injury. Chronic ankle spains can stretch it and cause scar tissue to form against it. If injured, you will experience difficulty walking and numbness in the exact area you describe. The treatment/cure for this is ice over the spot described above and manual manipulation of the proximal head of the fibula by a Chiropractor.
Many D.C.'s are unable or not trained to do extremity adjusting, so you have to find one that does.
If you give me your location, I can find a competent physician to treat you.
The poor signal on the knee MRI helps pinpoint the area of interest but doesn't tell all.
No secret here, you just need to find the right tool for the job.
Let me know and over the weekend and Monday I will find you someone that knows what they are doing. A EMG often won't pick this up either.
Here is a refresher course for your neurologist, he may benefit from the following.
Anatomy
The superficial peroneal nerve travels in the lateral compartment and supplies the peroneus longus and brevis muscles. In most individuals at approximately the level of middle and lower thirds of the leg and at an average of about 10-15 cm above the tip of the lateral malleolus, the superficial peroneal nerve pierces the deep fascia and emerges into the subcutaneous fat. An average of 4-6 cm proximal to the ankle joint, it divides into a large (2.9 mm) medial dorsal cutaneous and a smaller (2 mm) more laterally located intermediate dorsal cutaneous nerve.
In 28% of patients, the superficial peroneal nerve branches more proximally. In these cases, the medial dorsal cutaneous branch usually follows the more common track of the superficial peroneal nerve and emerges into the subcutaneous tissues in the distal lateral leg. The intermediate dorsal cutaneous nerve penetrates the crural fascia further distally either anterior or posterior to the fibula an average of 4-6 cm proximal to the ankle joint. At the level of the malleoli, in most patients, the medial dorsal cutaneous nerve is located at approximately half the distance from the lateral malleolus to medial malleolus, and the intermediate dorsal cutaneous nerve is at approximately a third the distance.
The medial dorsal cutaneous nerve supplies the skin of the dorsomedial aspect of the ankle, the medial aspect of the hallux, and the second and third digits (except the first web space). The intermediate dorsal cutaneous nerve supplies the skin on the dorsolateral part of the ankle and gives off dorsal digital nerves for the third, fourth, and fifth toes.
Accessory branches of the superficial peroneal nerve have been reported to cross over the lateral malleolus, where they have been entrapped by fascial bands. An accessory motor branch of the superficial peroneal nerve has also been found to innervate the EDB in some patients.
Etiology
Local trauma or compression is the most common underlying cause of entrapment of the superficial peroneal nerve. Certain positions, such as prolonged kneeling and squatting, over many years or repetitive ankle sprains can make certain individuals more prone to development of symptoms. This tendency is thought to be due to recurrent stretch injury to the nerve. Perineural fibrosis of the superficial peroneal nerve at the level of the ankle following an inversion ankle sprain has been reported.
This nerve is also at risk for direct injury by any procedure about the anterior ankle, including the anterolateral ankle arthroscopy portal. Chronic or exertional lateral compartment syndrome can also cause compression of superficial peroneal nerve, particularly in athletes.
Nontraumatic causes of entrapment are commonly due to anatomical variations such as fascial defects, with or without muscle herniation about the lateral lower leg, where the nerve is entrapped as it emerges into the subcutaneous tissue, or a short peroneal tunnel proximally.
Clinical
Although patients may present with numbness or paresthesia in the distribution of the nerve and occasionally have pain about the lateral leg, the most typical presentation is vague pain over the dorsum of the foot. The pain can be chronic and present for several years and may be associated with other foot and ankle symptoms, or the pain can be acute and associated with recent trauma or surgery about the ankle. The anterolateral arthroscopy portal, in specific, puts this nerve at risk for direct or stretch injury, as does noninvasive traction methods with straps over the dorsum foot. About one quarter of patients have a history of previous or recurrent ankle sprain or trauma.
Typically, symptoms increase with activity such as running, walking, and squatting, and rest or avoiding a specific activity often relieves the symptoms. This tendency is particularly pronounced in athletes whose symptoms are suggestive of exertional or chronic anterolateral compartment syndrome.
Bony entrapment of the superficial peroneal nerve in the fracture callus has also been reported when fractures of the fibula heal with abundant callus.
Certain positions, such as crossing the leg over the other thigh, can induce symptoms, as can tight clothing, such as sock elastic over the lateral leg. Pain may occasionally occur at night. Occasionally, patients report a bulging mass in the leg.
Examination should include the entire course of the nerve, starting from the lower back and extending through the sciatic notch, the proximal fibula, and the lateral leg, where a muscle bulge due to a facial defect may be palpated in some patients. Percussion along the superficial course of the nerve over the proximal fibula, lateral leg, or the anterior ankle may cause a positive result on Tinel test, with reproduction of radiating pain. Direct palpation with pressure on the site of entrapment may also induce or exacerbate symptoms. Repeating the examination after a particular activity that exacerbates symptoms may produce findings not present on the initial examination at rest.
In competitive athletes who have symptoms suggestive exertional compartment syndrome, Styf describes 3 provocative tests for nerve compression at rest and again at rest but after exercise. In the first test, pressure is applied over the anterior intermuscular septum while the patient actively dorsiflexes the ankle. In the second test, the foot is passively plantarflexed and inverted at the ankle. In the third test, while the patient maintains the passive stretch, gentle percussion is applied over the course of the nerve.
In some cases of superficial peroneal nerve entrapment associated with direct or indirect trauma, patients may present with symptoms of reflex sympathetic dystrophy (RSD)/complex regional pain syndrome (CRPS), which creates a diagnostic and therapeutic challenge.
Infrequently, weakness of the dorsiflexors and everters of the foot may be seen with associated foot drop in more proximal entrapments of the superficial peroneal nerve.
Although rare, plain radiographs of the leg may reveal bony abnormalities that may contribute or be the cause of entrapment. In cases of suspected proximal entrapment, knee radiographs may show abnormalities of the proximal fibula, such as exostoses, osteochondromas, and fracture callus. If necessary, a CT scan can provide more detailed information on the bony anatomy of the area, and a sonogram can help localize cystic masses that cause impingement of the nerve.
An MRI study is rarely necessary to obtain additional information.
Occasionally, in cases of exertional compartment syndrome, the measurement of the intramuscular pressure at rest after exercise may be helpful.
Injection of the nerve with lidocaine or Marcaine just above the site of involvement can be the most valuable diagnostic tool. The patient can define the extent of relief obtained from such an injection, which can be helpful in defining the zone of injury and expected relief from surgical release or excision.
The value of electrodiagnostic studies varies in the literature. Although many times findings from electrodiagnostic tests are normal because these dynamic syndromes frequently improve or resolve at rest, these tests may reveal an unrecordable evoked response or a prolonged distal latency of a segment of the nerve and help to better define the zone of compression. They also help in the evaluation of concomitant radiculopathy or peripheral neuropathy.
I am willing to bet if the doctor examines you with his hands and not a machine, he will find the exact location of entrapment in short order, I know I would. Just ask and I will have this taken care of promptly.
Dr. Timothy Durnin
drs.chiroweb.com
Dr. Timothy Durnin
drs.chiroweb.com