Tibial tuberosity fractures are infrequent fractures affecting physically active adolescents.[1, 2, 3, 4, 5] Activities involving powerful contraction of the knee extensors, such as springing and jumping movements, can result in avulsion fractures of the tibial tuberosity apophysis.[6, 7, 8] This condition should be distinguished from Osgood-Schlatter disease, a chronic apophysitis of the tibial tuberosity due to recurrent traction injury.
Nondisplaced type I injuries can be managed conservatively by cast immobilization in a long leg cast in full-knee extension. All other injuries are best treated by open reduction and internal fixation with cast immobilization for 6-8 weeks. (See Treatment.)
NextThe extensor complex of the thigh exerts its force through the ligamentum patellae on the tibial tuberosity. During its histogenesis, the tibial tuberosity is an anterior extension of the proximal tibial epiphysis separated from the rest of the tibia by the growth plate. As the growth plate closes in late puberty, it is transiently replaced by fibrocartilaginous elements, which predispose it to traction injury as a result of its weaker tensile strength.
The proximal tibia has two ossification centers, the proximal tibial epiphysis and the tibial tuberosity, which are separated by a cartilage bridge (see the image below). Before ossification, the tibial tuberosity is composed of fibrocartilage that has good tensile strength. However, during ossification, columnated cartilaginous cells with poor tensile strength replace the fibrocartilage, and it is within this small window between fibrocartilage and ossified matrix that the tibial tuberosity is at risk of avulsion fractures.
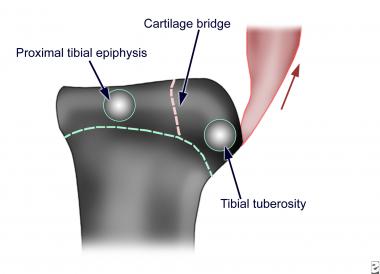 Ossification centers and epiphyseal cartilages of the proximal tibia and tibial tuberosity.
Ossification centers and epiphyseal cartilages of the proximal tibia and tibial tuberosity. As a result of the direction of pull of the patella tendon, the tibial tuberosity along with the proximal tibial epiphysis can be avulsed upward in a fracture in one or more fragments (see the image below).
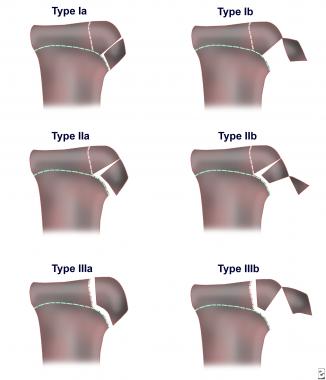 Classification of tibial tuberosity fractures.
Classification of tibial tuberosity fractures. Watson-Jones classified the fractures into the following three types[9] :
Ogden modified this classification by adding the subtypes A and B,[10] with A representing single fractures and B representing comminuted fractures.
Tibial tubercle fracture is caused by injury from violent tensile forces on the tibial tuberosity. The force is delivered through eccentric contraction of the extensor mechanism of the knee from either of the following:
In other words, it occurs when sudden acceleration or deceleration of the extensor mechanism occurs.
Patients with Osgood-Schlatter disease may be predisposed to tibial tuberosity fractures.[11] Similarly, patients with these fractures may have a family history of Osgood-Schlatter disease or a history of fractures of the tibial tuberosity.
In the United States, the frequency of tibial tubercle fracture has not been determined, though the injury is known to occur infrequently. At one major center, 15 cases of tibial tuberosity fractures were diagnosed in 5 years. Tibial tuberosity fractures typically occur in individuals aged 14-17 years. As the growth plate closes in late puberty, it is transiently replaced by fibrocartilaginous elements. These elements predispose the tibial tuberosity to traction injury as a result of its weakened tensile strength.
Internationally, the frequency is not known. As in the United States, the condition occurs infrequently.
Clinical Presentation
Copyright © www.orthopaedics.win Bone Health All Rights Reserved


