In 1914, Alfred H Freiberg first described the painful collapse of the articular surface of the second metatarsal head.[1] He reported six cases of young women presenting with a painful limp and discomfort localized to the second metatarsal. All six patients had similar radiographic findings, which showed collapse of the articular surface of the second metatarsal head. In three patients, intra-articular loose bodies were seen. Of the six women, four were younger than 18 years.
Because Freiberg believed that the etiology most likely was trauma, he used the term infraction.[1] He postulated that the condition was partially caused by excessive length of the second metatarsal. He believed that a long second metatarsal combined with an ineffective first ray complex led to an overload of the second metatarsal and subsequent articular collapse.
Since Freiberg's original description, multiple authors have written about this uncommon condition, which has since come to be known as Freiberg disease (first described as Freiberg infraction but also referred to as Freiberg infarction).
NextThe true incidence of Freiberg disease has not been established. Some cases are asymptomatic, and others may resolve spontaneously before treatment is sought. Freiberg disease appears to be an uncommon condition, as evidenced by the small number of patients in most series that are reported in the literature.
Consistent with Freiberg's original description, the disease most commonly is seen in young women. In a review of 275 reported cases, Katcherian found an overall male-to-female ratio of approximately 1:5.This female preponderance is unusual among the osteochondroses as a whole, in which males are more affected.[2]
In more than 95% of cases, the lesion is found in the second or third metatarsal, with the second metatarsal being affected more often. However, any of the metatarsals may be involved, though the first and fifth are rarely affected.[3] Almost always, there is a single lesion in one foot. Bilateral involvement has been reported to occur in fewer than 10% of patients.[4]
The individuals most commonly affected range in age from adolescence through the second decade of life. However, Freiberg disease can occur at any age, with an age range of 8-77 years reported in the literature.
In his original description, Freiberg favored a traumatic etiology; however, he admitted that trauma itself could not reliably explain all cases.[5] Despite several thoughtful investigations into the etiology of Freiberg disease, no consensus exists as to what type of disease process this peculiar affliction represents. This lack of consensus is reflected in the numerous terms used in the literature to describe this process.
Freiberg disease in adolescents is thought to belong to a group of related diseases involving growth disturbances of the epiphysis or apophysis, collectively termed the osteochondroses. Although it is considered to represent an interruption of normal growth processes, the specific events or factors that incite the cascade leading to articular collapse are unclear. Among the more common articular osteochondroses are Köhler disease of the tarsal navicular, Legg-Calve-Perthes disease of the femoral head, and Panner disease of the humeral capitellum.[6]
Although regarding Freiberg disease as an osteochondrosis makes sense, it does not fully explain the adult-onset form of the disease, which may reflect a different process altogether, albeit radiographically similar one. Some authors consider the cause to be multifactorial. Unlike other osteochondroses, Freiberg disease is not commonly associated with steroid use, alcoholism, or smoking. Most current theories center on whether the initial insult is primarily traumatic or vascular. Infection has essentially been eliminated as a significant factor.
Radiographic changes consistent with avascular necrosis have led some authors to suggest that the inciting event is an injury to the vascular supply to the metatarsal head. Whether this is the result of a direct vascular injury or of repetitive injury to an area that has an inherently poor blood supply is unknown. Disorders that may affect blood supply (eg, diabetes mellitus, systemic lupus erythematosus, and hypercoagulability) have been suggested factors in the development of Freiberg disease.[7]
To better understand the blood supply to the metatarsal heads, several cadaveric investigations have been performed. Huber described the variability of the dorsal arteries in 200 feet, finding that 65% of those feet exhibited limited collateral anastomosis.[8] Leung and Wong described as many as seven different patterns of supply originating from the first webspace dorsal artery.[9]
Wiley and Thurston noted variation, finding that 33% of specimens studied lacked a second metatarsal artery, with collaterals from the first and third metatarsal arteries supplying the second metatarsal head.[10] Viladot and Viladot noted that the metatarsal head receives its vascular supply from small penetrating vessels at the joint capsule.[11]
These studies demonstrated that the vascular supply to the metatarsal heads can be quite variable. Overall, there appears to be a trend in which the second and third metatarsals receive a less consistent blood supply than the other metatarsals do. These studies may suggest that some patients may have a greater risk for the development of Freiberg disease based on their anatomic variances.
Others have cited reports of iatrogenic avascular necrosis of the second and third metatarsal heads following elective forefoot surgery as indirect evidence that a disturbed blood supply may be at least partially responsible for the development of Freiberg disease.[12]
Some authors, however, favor trauma as the predominant etiologic agent in the development of Freiberg disease, whether in the form of a single acute injury or in the form of multiple repetitive microinjuries. Various authors have suggested that altered kinematics around the forefoot may predispose some patients to injury as a result of abnormal loading and may ultimately contribute to the development of Freiberg disease.[13, 14] Several different local mechanical factors have been implicated.
One anatomic variant often implicated in Freiberg disease is a long second metatarsal. In his original description, Freiberg postulated that a long second metatarsal in combination with altered first ray mechanics eventually leads to overload of the second metatarsophalangeal (MTP) joint. He theorized that with forcible impact in feet predisposed by weakness of the toe flexors (especially the first toe), the longer second toe would be susceptible to injury. However, he did note that only four of his six original cases had a discrete history of trauma.[1]
Similarly, in their evaluation of various etiologic factors implicated in Freiberg disease, Stanley et al found that as measured from standing radiographs, the affected ray was the longest in 85% of the feet.[13] The authors believed this finding to be important. They noted that only five of 33 feet (15%) in their study had a discrete history of trauma.
Of the metatarsals, the second and third are the least mobile. This has led some investigators to conclude that these metatarsals, because of their relative inflexibility and increased load transmission, are at increased risk for sustaining repetitive microtrauma. Similarly, Smillie considered Freiberg disease to be a repetitive stress injury, analogous to a march, or stress, fracture.[15] He believed that concentration of stress in the trabecular bone at the dorsal aspect of the metatarsal head eventually leads to collapse.
In their summary of various etiologic factors, Stanley et al evaluated pressure under the metatarsals in patients diagnosed with Freiberg disease, finding that only five of 33 feet showed abnormally high pressures at the affected site.[13] However, in 16 patients (48%), the greatest measured pressure was indeed at the site where Freiberg disease was present.
McMaster proposed a possible mechanism of injury for the development of Freiberg disease.[16] On the basis of similarities between lesions observed in hallux rigidus and Freiberg disease, he suggested that the typical location of the lesions could be explained on the basis of mechanical impingement between the base of the proximal phalanx and the dorsum of the metatarsal head in forced dorsiflexion. He postulated that the relative inflexibility of the second and third metatarsals contributed to the development of lesions at these particular sites.
In an attempt to test this hypothesis, Helal and Gibb induced joint incongruity by creating artificial effusions.[17] Viscous silicone was injected into the MTP joints of cadaveric feet. Joint congruity was then radiographically assessed in varying degrees of dorsiflexion and plantar flexion.
Helal and Gibb observed dorsal impingement of the metatarsal head and the proximal phalanx under these conditions.[17] They attributed the dorsal impingement to joint incongruity induced by the effusion. They believed that the impingement occurred dorsally because the MTP joint capsule is inherently thicker dorsally than it is ventrally. However, whether or not an effusion plays a significant role in the development of Freiberg disease in vivo is unclear.
In an attempt to evaluate trauma in the development of Freiberg disease, Braddock subjected intact cadaveric second MTP joints to axial loads. In two of the 10 specimens, he was able to create lesions closely resembling those seen in Freiberg disease. The stage of epiphyseal maturation in the two specimens resembled that commonly seen in adolescent-onset Freiberg disease. This led him to conclude that trauma to the second metatarsal at the proper phase of epiphyseal maturation could produce lesions similar to those of Freiberg disease.[18]
Others have considered the disorder's predilection for women to be indirect evidence that trauma plays an etiologic role. Theories are based on male-female differences in the selection of shoe wear; presumably, high-heeled shoes subject the metatarsal heads to repetitive injury and increased pressure transmission. Hoskinson reported the development of Freiberg disease in three females after initial attempts at wearing high-heeled shoes.[19] Anecdotal experience aside, there is no direct evidence linking the disease with the wearing of high heels.
Nguyen et al observed seven cases of Freiberg disease occurring in older patients with diabetes.[20] They questioned whether trauma to the metatarsal heads as an indirect result of a peripheral neuropathy could result in the development of Freiberg disease. They postulated that intrinsic motor weakness, such as is often seen with peripheral neuropathy, can lead to extension of the toes at the MTP joint, resulting in an increase in weightbearing by the metatarsal heads, repetitive injury, and subsequent collapse.
Of the seven patients studied by Nguyen et al, three had a documented neuropathy.[20] The authors did not comment on whether the patients had protective sensation or if changes of Charcot arthropathy were present in the other joints of the foot.
In summary, the exact nature of the etiology of Freiberg disease is unknown. It is most likely multifactorial, including vascular and traumatic insults. Certain patients may be anatomically predisposed by mechanical, vascular, and developmental factors. Whether the process is the same for older patients as it is for adolescents is unknown.
The relative infrequency of the disease, as well as the variable presentation regarding age and injury, makes the study of various etiologies challenging. In the future, genetic or other variables that play a role in the development of Freiberg disease may be identified. Further investigation is needed.
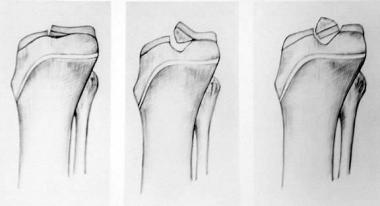
In its juvenile osteochondrosis form, Freiberg disease is a degenerative process involving the epiphyses resulting in osteonecrosis of subchondral cancellous bone. If the process is altered in such a way as to restore normal physiology, this may be followed by regeneration or recalcification. If not, the process continues to subchondral collapse and eventual fragmentation of the joint surface.[21]
Patients typically present with complaints of activity-related forefoot pain. Walking alone is often sufficient to cause pain. Some patients describe a chronic (months to years) history of forefoot pain with episodic exacerbation, whereas others present with a recent onset of pain related to a specific injury or event. A history of trauma may not be noted. Patients may present with stiffness and a limp. The pain is often vague and poorly localized to the forefoot. Some patients describe the sensation of a small, hard object under the foot.
Physical examination typically reveals a limited range of motion (ROM), swelling, and tenderness with direct palpation of the MTP joint. In early stages of the disease, MTP tenderness may be the only finding. In later stages, crepitus or deformity may be present. A skin callus may be seen on the plantar surface of the affected metatarsal head.
The most common differential diagnoses include metatarsalgia, Morton neuroma, stress fracture of the metatarsal, and synovitis.
Whereas some stage I, stage II, and stage III lesions (see Staging) may resolve spontaneously, patients who do not respond to conservative measures may require surgery, as may patients with stage IV and stage V lesions.
Conservative management is recommended in the pediatric population and in patients with early-stage lesions. Otherwise, no true contraindications to treatment of Freiberg disease exist.
Workup
Copyright © www.orthopaedics.win Bone Health All Rights Reserved