Dislocation of the ankle usually occurs with fractures of the malleoli or of the posterior aspect of the tibia because the ankle’s ligamentous structures are, in most cases, stronger than the osseous architecture. In addition to a strong association with fractures, ankle dislocations are often open because of the thin layer of tissue that lies over the malleoli. Posterior dislocation of the talus is the most common form of ankle dislocation, though medial, anterior, lateral, and superior dislocations have been well described.
Individuals at increased risk for ankle dislocation injuries include those with a history of prior ankle fractures, ankle sprains, weakness of the peroneal muscles, malleolar hypoplasia, or ligamentous laxity such as may occur with Ehlers-Danlos syndrome and other connective tissue disorders.
An ankle dislocation represents a high-force traumatic injury that often occurs in vehicular collisions or sports that involve jumping. The clinician must, therefore, examine the patient thoroughly for additional injuries.
The energy of the traumatic insult usually either forces the ankle into a position of plantar flexion or strikes the ankle while it is already in a resting position of plantar flexion. Once in plantar flexion, all capsular ligaments of the ankle (with the exception of the posterior talofibular ligament) are stretched and, therefore, more susceptible to structural failure. In addition, plantar flexion brings the smaller surface area of the posterior edge of the talus into the mortise of the ankle, which makes translational forces on the talus more likely to dislodge it from the joint.
Injuries that cause subsequent inversion of the ankle lead to posteromedial displacement and tears in the anterior talofibular and calcaneofibular ligaments. Eversion injuries are more likely to produce lateral dislocations and rupture of the talotibial ligament and medial joint capsule. Inversion injuries are more common as a result of axial loads from falls from significant height.
The rupture of the ankle’s capsular structures is often severe, and the risk of infection secondary to open injury is often significant; however, prompt reduction and, when warranted, operative debridement and repair usually lead to excellent functional recovery and long-term prognosis. Immediate recognition and early reduction of the dislocated ankle are essential, in that delayed reduction may lead to subsequent loss of range of motion and increased morbidity.
Evaluation of the ankle injury must sufficiently demonstrate that the dislocation is of the ankle joint; subtalar dislocations may have presentations similar to those of dislocated ankles but are reduced with a different method.[1, 2] Applying the ankle reduction technique to a subtalar dislocation may lead to further injury and morbidity, and the two injuries may be clearly differentiated from each other radiographically. In addition to aiding in initial diagnosis, radiography helps to identify the anatomy of the fractures associated with ankle dislocations and should be performed both before and after reduction.[3]
NextReduction is indicated for the following:
Subtalar dislocations are rare (<2% of large-joint dislocations) and are the result of high-force mechanisms of injury directed at the forefoot. Of note, 10-20% of subtalar dislocations are irreducible by closed methods and require operative intervention. Radiographs of the ankle, including anteroposterior (AP), lateral, and mortise views, may quickly and reliably differentiate between ankle and subtalar dislocations.
Contraindications include the following:
As noted, it is essential to differentiate an ankle injury with dislocation from a subtalar dislocation (see Table 1 below).[1] An attempt to reduce a subtalar dislocation with ankle reduction techniques is likely to be unsuccessful and may lead to further injury of the involved articular structures.
Table 1. Differentiating Features for Ankle Dislocation and Subtalar Dislocation (Open Table in a new window)
Ankle (Tibiotalar) Dislocation Subtalar Dislocation Malleoli tent or perforate the skin Talar head tents or perforates the skin Deformity is proximal; ankle and foot remain aligned Deformity is more distal; ankle and foot are malaligned Foot is rarely held in a position of inversion or eversion Foot is often held in a position of inversion or eversionIsolated subtalar dislocations have been reported.[4] Lateral subtalar dislocations are rare but have been reported; these can also occur with bimalleolar fractures.[5]
The ankle is a unique modified saddle joint that, together with the subtalar joint, provides range of motion in several physical planes while maintaining stability. The ankle's complex function as a pivoting structure positioned to bear almost the entire weight of the body leaves it vulnerable to tremendous forces of injury. Pure dislocation without associated fracture was once thought to be rare[6] ; however, several cases of isolated ankle dislocation without fracture have been reported.[7, 8, 9, 10, 11, 12, 13]
The combined movement in the dorsiflexion and plantarflexion directions is greater than 100°; bone-on-bone abutment beyond this range protects the anterior and posterior ankle capsular ligaments from injury. The anterior and posterior ankle capsular ligaments are relatively thin in comparison with the medial and lateral ankle ligaments. (See the image below.) For more information about the relevant anatomy, see Ankle Joint Anatomy.
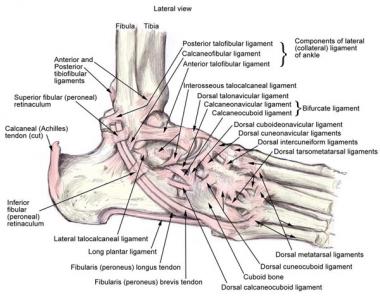 Anatomy of the lateral ankle ligamentous complex and related structures.
Periprocedural Care
Anatomy of the lateral ankle ligamentous complex and related structures.
Periprocedural Care
Copyright © www.orthopaedics.win Bone Health All Rights Reserved