QuestionI developed scoliosis which was visible at age 14. At that time, I had a corset brace with a bar under my right arm which I eventually did not use because of uncomfort and unsightly appearance. Of course the scoliosis got worse; I am now 65 years old and, although it is not noticeable in the front, there is a bump in my back on the right side which effects by left rib cage. Any twisting or lifting of heavy objects, and the pain is indescribably unbearable. I had physical therapy several years ago which included massages and stretching exercises. Those massages helped me so much and the spinal doctor wrote out a prescription for the massages. The physical therapy center refused to honor the prescription because they felt "they were not massage therapists". I don't believe that any insurance plans would pay for massages, they consider that a luxury. The only way I can relieve the pain is by taking 3 ibuprofen with a heating pad, the pain always subsides after 3 days. They told me not to see a chiropractor, I was wondering why? Any suggesting would be greatly appreciated.
AnswerStaten Island Scoliosis, Scoliosis/Rib cage pain,
Hello Sandra,
I am sorry to hear of your complaints.
I have some preprinted information which I utilize with my Staten Island Scoliosis patients, this may be helpful to you:
Scoliosis
Everyone's spine has a natural front-to-back curve -- that's what produces the normal rounding of the shoulders and the sway of the lower back.
However, some people suffer from "Scoliosis" ?an abnormal curvature of the spine, especially one characterized by a rotational side-to-side deformity.
In simple terms, what this means is that the spine is twisted side-to-side, often taking on an "S" shaped appearance and even resembling a corkscrew in some cases.
Almost three out of every 100 people have some degree of abnormal spinal curvature, and for some it never becomes a serious problem. But for many others, the curve gets worse over time and can cause considerable pain, frustration, and limitations on normal activities.
Severe scoliosis can even complicate breathing and circulation.
The current medical approach to scoliosis is to react to symptoms of curve progression, not to prevent potential progression. It is mainly a "wait and see" attitude - yes, you have it, but we'll just watch it for a while and when it starts to get worse, we'll do something!" However, according to the Journal of American Family Physicians, 1999, underarm thoroco-lumbar-sacral orthosis (TLSO) braces have a 74 percent success rate in slowing curve progression.
According to the AAOS figures, almost all cases of juvenile scoliosis (in children ages 3-10) progress.
This group accounts for 15 percent of the scoliosis cases. Fifty percent of the cases progress to a point of surgical intervention. Adolescence scoliosis (in children older than age 10) comprises 80 percent of scoliosis in children, and 5 percent to 25 percent of these cases progress. The AAOS further states that if the curve is greater than 20 degrees at 10-12 years of age, there is a 68 percent chance it will progress. The AOS also concurs that even after bone maturity, especially in curves greater than 30 degrees, some progression occurs.
Who suffers from scoliosis?
The most common form of scoliosis is called idiopathic scoliosis, which basically means that the cause is unknown. Anyone can suffer from scoliosis; the condition usually begins in childhood, although too often it is not identified until the teenage years or later.
Scoliosis tends to run in families, and it affects many more girls than boys. In fact, research indicates that girls are nearly eight times more likely than boys to have scoliosis and five times more likely to require some form of treatment for their condition than boys, and the curvature of their spine is more likely to worsen over time, especially if left unattended.
What are some of the symptoms of scoliosis?
Sometimes curvature of the spine is visible (the body tilts to the left or the right, or one shoulder blade is raised higher than the other. Some of the actual physical symptoms of scoliosis can include back pain, fatigue (especially postural fatigue -- feeling tired when standing, sitting, etc.), and in more severe cases, problems with circulation and breathing.
What can chiropractic do?
Doctors of chiropractic are trained to identify and manage problems relating to the spine and the back. An initial visit to the chiropractor will include a thorough physical and diagnostic examination (including range-of-motion tests and spinal x-rays) to identify any problems you may be having, including whether you or your children may be suffering from abnormal or dangerous curvature of the spine.
If you do show signs of scoliosis, your chiropractor can provide a variety of techniques to help your condition, including spinal adjustments to increase movement and biomechanical function, and advice on posture and exercise to help prevent further increase in the problem.+++++++++++++++++++++++++++++++++++++++++++
Scoliosis and the Chiropractic Approach http://www.planetc1.com/chiropractic-articles/scoliosis-chiropractic.html
By Matthew Trull
Analysis of Findings
Scoliosis can be very serious. If detected early, the chances for stabilization and reduction of the curves are very good. In my family alone, we have two examples. My sister抯 Scoliosis was diagnosed when both her curves had already progressed to 45 degrees. She had Spinal Fusion surgery in Atlanta at Scottish Rites Children抯 Hospital. The surgery was successful; her curves were reduced to 20 degrees each. However, it was very dangerous, painful, expensive, and changed her life dramatically. My Scoliosis was diagnosed early, while I had only one curve that was 21 degrees. Following six months of Chiropractic care, I have been completely cured of Scoliosis. The approach was painless, inexpensive, and did not alter my life in any way. I believe Chiropractic care should be the first-line approach for all patients diagnosed with Scoliosis. My research has proven it has a very high success rate: 70% achieving stabilization and reduction, and 15% obtaining total correction!
Typical Treatment Options
Bracing: For curves 30-degrees or less, a Milwaukee brace is typically worn. It is a rigid brace that exerts pressure against the spine, in hopes of achieving stabilization. The brace is uncomfortable, unsightly, and is usually worn 20-24 hours per day, until the patient stops growing. It offers no correction, and is only marginally effective for stabilization.
Surgery: An orthopedic surgeon performs Spinal Fusion surgery. The patient is placed on a spinal cord monitor to prevent paralysis. After performing an incision, the surgeon manually reduces the curves as much as possible, and inserts metal rods on each side of the spine, attaching them with special hardware. Bone splinters (either removed from the hip area, or donor bone) are applied between the vertebrae. Over time, these fragments grow together to create a solid bone. Surgery is very expensive, painful, dangerous, and requires the patient to alter their lifestyle forever. Surgery is very effective for reducing curves. Surgery should be considered a last resort.
Signs of Scoliosis
Most obvious signs of Scoliosis are: shoulders of unequal height, a 憆ib hump? which is caused by the ribcage on the back protruding more on one side than the other, and hips that appear unequal in height. Scoliosis clinics are conducted free of charge by health Departments and Chiropractors. A school or Health Department nurse or Physical Education teacher routinely screens students during the middle school years. It is extremely important to diagnosis and treat Scoliosis as early as possible.
Special Thank-You
I want to thank Dr. Marc Schnobrich, of Rincon Chiropractic, for all the many ways he has helped my family and me. He diagnosed my Scoliosis while treating me for an elbow injury. During the following months, he treated me weekly, always explaining what he was going to do. He provided excellent chiropractic care in many other areas, as well. Dr. Marc checked my spine often for progress. After six months of care, I was completely cured!
Dr. Marc has always been very kind, caring and helpful. He has been my friend as well as my doctor! During my research for this project, he loaned me books and other research materials. He patiently answered questions, and was never too busy to talk to me on the telephone between visits. He also answered my emails promptly and accurately. Thanks to Dr. Marc抯 care, I will be able to continue my normal lifestyle, which includes baseball and many other physical activities.
Thank you, Dr. Marc!
Conclusion
Spinal Fusion surgery is very painful, expensive, and will alter the lifestyle of the patient forever. Surgery should be considered the last alternative in treating Scoliosis. Wearing a Milwaukee Brace is uncomfortable, limits physical activity, offers no correction, and is mostly ineffective in stabilizing the spine. The Chiropractic approach is very effective at stabilizing the spine, preventing the curve from progressing. At least 70% of the patients achieve some degree of reduction in the size of the curves. Approximately 15% of Scoliosis patients achieve total correction, like I did! That means at least fifteen out of 100 patients will not have to face surgery, take medications, and change their lifestyle forever! All of this is done with a minimum of cost and no pain! Research and experience have proven Chiropractic care is definitely effective in the stabilization and reduction of Scoliosis!
Chiropractic care should be the first-line approach for all Scoliosis patients.
Chiropractic Facts
The first Chiropractic adjustment performed on the North American Continent was in 1895, by Dr. Daniel David Palmer. His first patient experienced deafness following a back injury. Following care, the patient reported improved hearing. Dr. Palmer founded the Palmer School of Chiropractic in Davenport, Iowa, which continues to train Chiropractors today.
Spinal manipulation has been practiced since the beginning of recorded time. Over 2700 years ago the Chinese documented this form of treatment. Records indicate that ancient Japanese, Indians, Egyptians, Babylonians, Syrians, Tibetans, and Native Americans practiced a hands on approach to health.
An estimated 19.5 million Americans visit a Chiropractor each year.
There are over 50,000 licensed Chiropractors in the United States, and another 30,000 worldwide.
Chiropractic is the world's second largest health care profession. It promotes the body抯 own ability to heal itself. Chiropractic uses no drugs or surgery, and is all-natural.
Evaluation of Work
I believe whole-heartedly in Chiropractic Care for Scoliosis. I am living proof that it works! I thoroughly enjoyed researching this project. I was eager to find if others had similar success. I was delighted to find that more than 2/3 of the Scoliosis patients seeking Chiropractic care had very good results. It was fascinating to speak with Chiropractors who treat Scoliosis on a regular basis. I found them to be very caring, dedicated professionals. I accompanied my sister to Atlanta for her Spinal Fusion surgery, and remember the excruciating pain she suffered. I see her daily life changed. I wish my parents had been aware of Chiropractic when my sister was diagnosed with Scoliosis. Maybe next year I抣l research why more health care professionals don抰 offer Chiropractic care as an option to their Scoliosis patients. More public education is definitely needed in this area!
Scoliosis-
is an OBVIOUS Misalignment of the spine.
The spine compensates- like dominoes - - - one falls here, and the final domino may be far distant !, Like the old song- the toe bones connected to the foot bone, the foot bone to the ankle bone, the ankle bone is connected to the leg bone, the leg bone is connected to the knee bone, etc etc etc. the body is all interconnected and interdependent. A misalignment (subluxation) in the spine can cause a compensation elsewhere contributing to an abnormal curvature- known as a SCOLIOSIS.
Scoliosis: a misalignment of the SPINE often contributed to by:
Vertebral Subluxation Complex (a.k.a. 憇ubluxation?
The vertebral subluxation complex is the underlying cause of many healthcare problems.
The kinesiopathology of the subluxation (misalignment, improper movement pattern) is often involved with scoliosis, and can sometimes be the cause of the curvature.
A subluxation interferes with the proper functioning of joints, and can cause scoliosis, osteo-arthritic degeneration, Degenerative Disk Disease, degenerative joint disease, etc.
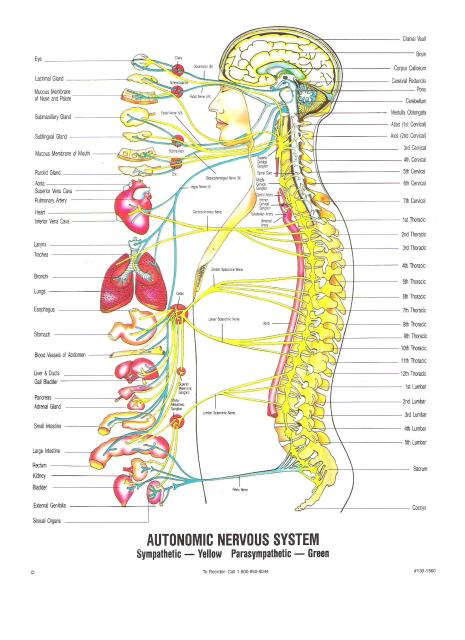
A subluxation interferes with the proper functioning of the nervous system (the master system which controls and coordinates all function within the body- i.e.: muscles) and may cause various other conditions, symptoms and problems.
Subluxation is a serious condition identified by its five parts:
Spinal Kinesiopathology:
This is fancy way of saying the bones of the spine have lost their normal motion and position. It restricts your ability to turn and bend. It sets in motion the other four components.
Neuropathophysiology:
Improper spinal function can choke, stretch, or irritate delicate nerve tissue. The resulting nerve system dysfunction can cause symptoms elsewhere in the body.
Myopathology:
Muscles supporting the spine can weaken, atrophy, or become tight and go into spasm. The resulting scar tissue changes muscle tone, requiring repeated spinal adjustments.
Histopathology:
A rise in temperature from an increase in blood and lymph supplies result in swelling and inflammation. Inflammed Discs can easily bulge, herniate, tear, or degenerate. Other soft tissues may also suffer permanent damage.
Pathophysiology:
The VSC contributes to OsteoArthritic degeneration. Bone spurs and other abnormal bony growths attempt to fuse malfunctioning spinal joints. This spinal decay, scar tissue, and long-term nerve dysfunction can cause other systems of the body to malfunction.
The Vertebral Subluxation Complex describes what happens when spinal bones lose their normal movement patterns and position. When subluxated, joints are in a stressed, vulnerable, compromised condition. Vertebral Subluxation may cause Spinal Scoliosis, Arthritis, Disk Herniation, Disk Degeneration, or aggravate such conditions.
Vertebral Subluxation cannot be corrected through chemicals (medicine), stretching, yoga, vitamins or physical therapy alone. Subluxation- a neuro/skeletal/muscular- mechanical- problem requires a mechanical correction- - - a manipulation, best performed with the chiropractic adjustment by Doctor of Chiropractic. Scoliosis??- nothing better then the CHIROPRACTIC Adjustment. Plus- do your at home exercise (ie 慼anging? as instructed.
Dr. Victor E. Dolan, Doctor of Chiropractic; Diplomat, American Chiropractic Board of Sport Physicians; Diplomat, American Academy of Pain Management; Certified Clinical Nutritionist (IAACN); FIRST Chief of Chiropractic in a Hospital in New York State (DHSI); As Seen in PREVENTION Magazine
I hope that article above helps,,,,,,,,,,
You also state you take Ibuprofen (NSAID), this information may help you as well:
PAIN
Pain is a 憆ed light on the dashboard?
Pain is your body telling you that something is wrong.
That RED LIGHT on the dashboard of your car-
-- do you ignore it until the car breaks down,
or do you get it checked and correct the problem?
Pain,
pain in your body-
-- do you ignore it until your body breaks down,
or do you get it checked and correct the problem?
Pain,
do you cover up the pain by taking a painkiller?
Take a painkiller,
mask the pain,
and allow a problem to progress in your body?
NOTICE ON PAIN RELIEVERS:
Label changes ORDERED by FDA; the FDA announced proposed label changes for OTC over-the-counter pain relievers to include the potential for stomach bleeding and liver damage (FDA news 206- 207; 12-9-06) ;
The American Heart Association issued a scientific statement recommending medical doctors change the way they prescribe OTC pain relievers from a first choice to an alternate of recommending non-pharmacologic treatment (AHA statement 2-26-07).
NSAID Acceleration of ARTHRITIS; an important side effect of Aspirin and other NSAIDS is that it will inhibit cartilage repair and accelerate cartilage destruction ( Journal of Rheumatology, 1982; 9: 3- 5 ). Many times people take NSAIDS for the pain of Arthritis, not realizing these drugs may make the underlying condition worse. These medications cover up the pain, and cause the problem to worsen.
Pain can often be the result of the Vertebral Subluxation Complex.
Vertebral Subluxation ( 慥SC?, 憇ubluxation? )
Vertebral Subluxation is actually a quite common condition.
Doctors of Chiropractic look for pathological conditions which may require referral to other specialties, and also look for 慡ubluxation? Other disciplines look for pathology, but overlook the importance of alignment and movement in the spine which affects our nervous system (the master control system- ALL health disciplines learn this). VSC- 慡ubluxation??can be the cause of many symptoms and conditions.
Only a Doctor of Chiropractic will evaluate and treat for VSC, as well as other pathology.
The course of VSC is highly variable. Some patients with VSC literally cannot walk, yet other patients with similar test findings may be able to run marathons or lift heavy weights. Some patients immediately develop symptoms related to the VSC, some patients take years to develop symptoms. Some people suffer for only a few days with pain and symptoms, some people suffer for months. Some people recover in days, some take months or years, depending upon severity of the condition.
A subluxation interferes with the proper functioning of the nervous system (the master system which controls and coordinates all function within the body) and may cause various other conditions, symptoms and problems.
The Vertebral Subluxation Complex describes what happens when spinal bones lose their normal movement patterns and position. When subluxated, joints are in a stressed, vulnerable, compromised condition. Subluxation may cause Arthritis, Disk Herniation, or aggravate such conditions.
Vertebral Subluxation cannot be corrected through chemicals (medicine), stretching, yoga, vitamins or physical therapy alone. Subluxation- a neuro/skeletal/muscular- mechanical- problem requires a mechanical correction- - - a manipulation, best performed with the chiropractic adjustment.
Dr. Victor E. Dolan, Doctor of Chiropractic; Diplomat, American Chiropractic Board of Sport Physicians; Diplomat, American Academy of Pain Management; Certified Clinical Nutritionist (IAACN); FIRST Chief of Chiropractic in a Hospital in New York State (DHSI); As Seen in PREVENTION Magazine
As you can see from the above information, you must be cautious with any medication that you take!
".....the pain always subsides after 3 days....."- interesting. Pain is a way that our body talks to us, a way our body cells, tissues, organs talk to our brain. Pain is a nervous system function, a nerve function. Over time,,, a problem may remain, but a nerve tires of sending the message, a nerve ADAPTS.
Have you ever stepped out of the house on a very sunny day and been TEMPORARILY blinded by the sunlight? The change in lighting is noted by the nerves (eyes) and the message sent. Initially the change is great and overwhelming, THEN the nerve ADAPTS. The sunlight remains, but the nerves (eyes) adapt, get used to this level of stimulation.
Have you ever walked into a room with loud music, loud convesation?
If you and I walked in together--- at first we could not hear each other in conversation without shouting. BUT, after a few minutes you and I could be talking almost normally- because our nerves (ears) have adapted to the noise level. Our ears (nerves) are no longer overwhelmed by the change in ambient noise.
Same with your scoliosis. Same with your pain.
After a few days- your changing scoliosis, causing nerves to take notice and fire and send messages ADAPT. The nerves stop sending the message. It does not mean things have gotten better, it may mean things are still bad, but we are used to it by now.
".....They told me not to see a chiropractor,....."- I find that strange. I am a Doctor of Chiropractic (obviously) and refer and receive referrals every day from my medical doctor colleagues.
In talking about good doctors, good procedures,
SAFE APPROACHES
towards health problems - some startling facts may be discovered. A landmark article gathered all of the PUBLISHED evidence on healthcare:
"""""Death by Medicine
By Gary Null, PhD; Carolyn Dean MD, ND; Martin Feldman, MD; Debora Rasio, MD;
and Dorothy Smith, PhD
Something is wrong when regulatory agencies pretend that vitamins are dangerous, yet ignore published statistics showing that government-sanctioned medicine is the real hazard.
Until now, Life Extension could cite only isolated statistics to make its case about the dangers of conventional medicine. No one had ever analyzed and combined ALL of the published literature dealing with injuries and deaths caused by government-protected medicine.
That has now changed.
A group of researchers meticulously reviewed the statistical evidence and their findings are absolutely shocking.4 These researchers have authored a paper titled ""Death by Medicine"" that presents compelling evidence that today's system frequently causes more harm than good.
This fully referenced report shows the number of people having in-hospital, adverse reactions to prescribed drugs to be 2.2 million per year.
The number of unnecessary antibiotics prescribed annually for viral infections is 20 million per year.
The number of unnecessary medical and surgical procedures performed annually is
7.5 million per year.
The number of people exposed to unnecessary hospitalization annually is 8.9
million per year.
The most stunning statistic, however, is that the total number of deaths caused by conventional medicine is an astounding 783,936 per year.
It is now evident that the American medical system is the leading cause of death and injury in the US. (By contrast, the number of deaths attributable to heart disease in 2001 was 699,697, while the number of deaths attributable to cancer was 553,251.5)
We placed this article on our website to memorialize the failure of the American medical system. By exposing these gruesome statistics in painstaking detail, we provide a basis for competent and compassionate medical professionals to recognize the inadequacies of today's system and at least attempt to institute
meaningful reforms.
Table 1: Estimated Annual Mortality and Economic Cost of Medical Intervention
Condition --------- Deaths ------ Cost ------ Author
Adverse Drug Reactions 106,000 $12 billion Lazarou, Suh
Medical error 98,000 $2 billion IOM(6)
Bedsores 115,000 $55 billionXakellis(7),Barczak (8)
Infection 88,000 $5 billion Weinstein(9), MMWR (10)
Malnutrition 108,800 ----------- Nurses Coalition(11)
Outpatients 199,000 $77 billion Starfield(12), Weingart(112)
Unnecessary Procedures 37,136 $122 billion HCUP(3,13)
Surgery-Related 32,000 $9 billion AHRQ(85)
Total Deaths:
783,936
Total Costs
$282 billion
(References posted after signature) """""
Insurance rates are a good way to evaluate risk. Chiropractic malpractice rates vary from a high of 1/10th of certain medical specialties, to a low of 1/100th of certain medical specialties.
In NYC (the high cost district) Chiropractic Doctors usually
pay around $2000 per year for Millions of Dollars of coverage. I have heard medical malpractice premiums from $40,000 to $400,000 a year depending upon specialty and professional history.
I agree wholeheartedly with you, we must try to evaluate and look for the good doctors, good procedures, safe procedures.
Unfortunately the procedure of 'Manipulation' is often called 'Chiropractic'. It is not correct to call 'Manipulation' as 'Chiropractic', UNLESS a Doctor of Chiropractic applies the manipulation. If a 'manipulation' is performed by anyone other then a Chiropractor,,,, how can you call that 'chiropractic'?
I have done human dissection, I know my anatomy--- BUT if this chiropractor did 'surgery' upon a patient, I can guarantee a bad outcome, but should 'medicine' be penalized in malpractice or reputation?
If a different health profession(not chiropractic) performs a manipulation- and there is bad outcome, how can we lump that together with chiropractic. I belabor this point- because a few years ago a study came out purporting CHIROPRACTIC injury in 25 cases, upon researching the original data set it was discovered NONE of the manipulations were performed by DCs.
In Architecture there is a joke- the Medical Physician gets to bury their mistakes, the Architect can only tell the building owner to plant tall trees.
In Chiropractic School there is a joke- Every Chiropractor has someone telling people how the Chiropractor left them sore; the medical doctor has no complaints because he buries them.
I have also heard 'stories' at the cocktail parties about someone who had heard of someone injured by chiropractic. But I've never actually MET someone who has been injured by chiropractic. But people have heard stories.
I would direct you to
http://www.acatoday.org/pdf/ApprovedChiropracticSpecialtyPrograms.pdf Because
I appreciate continued education and dedication. I would recommend to you to Look for a Chiropractic Doctor near you with additional credentials, just as you would in any health field.
I do hope you view these:
Chiropractic Safety
http://www.youtube.com/watch?v=11VN2sGMdbI
Chiropractic works
http://www.youtube.com/watch?v=s68Yr38-lAQ&NR=1
interesting case history for you:
http://www.youtube.com/watch?v=qiOtb6yM_ow&NR=1
Myths:
http://www.worldchiropracticalliance.org/media/strokemyth.htm
Be aware- be careful if you take an NSAID for pain---
(1996): "Each year, use of NSAIDs (Non-Steroidal Anti-Inflammatory Drugs)
accounts for an estimated 7,600 deaths and 76,000 hospitalizations in the United States." (NSAIDs include aspirin, ibuprofen, naproxen, diclofenac, ketoprofen, and tiaprofenic acid.)
Source: Robyn Tamblyn, PhD; Laeora Berkson, MD, MHPE, FRCPC; W. Dale Jauphinee,
MD, FRCPC; David Gayton, MD, PhD, FRCPC; Roland Grad, MD, MSc; Allen Huang, MD,
FRCPC; Lisa Isaac, PhD; Peter McLeod, MD, FRCPC; and Linda Snell, MD, MHPE,
FRCPC, "Unnecessary Prescribing of NSAIDs and the Management of NSAID-Related
Gastropathy in Medical Practice," Annals of Internal Medicine (Washington, DC:
American College of Physicians, 1997), September 15, 1997, 127:429-438, from the
web at http://www.acponline.org/journals/annals/15sep97/nsaid.htm last accessed
Feb. 14, 2001, citing Fries, JF, "Assessing and understanding patient risk,"
Scandinavian Journal of Rheumatology Supplement, 1992;92:21-4.
---- remember, adverse drug events are probably UNDER-reported by at least a factor of ten.
"Do chiropactors have to "crack" my back?"
There are many different treatment
approaches in chiropractic (again, similar to medicine- I once read there were 55 different techniques to surgically remove hemorrhoids). Some techniques are 'low force'- some DCs feel these techniques are also lower in efficiency.
I do not know Chiropractic Doctors that 'crack' backs, I do know doctors that adjust backs--- similar to medical doctors who manipulate a frozen or dislocated shoulder. There are a thousand different chiropractic techniques in the hands of 70,000 different doctors. If you are interested in a chiropractic evaluation/ regimen- there should be some technique, some doctor that satisfies
your needs.
Speaking of different doctors, different techniques:
Sometimes, at a cocktail party, you may hear someone say,,, I tried a
chiropractor. ONCE. I'll never go back.
but
Do you ever hear; I went to a medical doctor. ONCE. I'll never go back.
What is the difference?
People switch medical doctors because of cost, bedside manner, location, parking, changing insurance, bad breath, lousy receptionist, too quick to cut, too slow to cut, too quick with prescriptions, too slow with prescriptions,
WHATEVER; , , , ,
, , , , but , , , they never say- that WHOLE profession of Medicine doesn't work; I'll never go back. and-- EVERYone I know has had at least one bad experience with some MD somewhere.
however......
Try one chiropractor. ONCE. not like it for any reason,,, and people can make a generalization about an entire licensed profession with 70,000 members, a thousand different approaches (and millions of satisfied patients- often the medical failures).
I find that kinda funny.
".....They told me not to see a chiropractor, I was wondering why?...." I simply cannot tell you why.
At this late date in the progression of your scoliosis there may be nothing a Doctor of Chiropractic can do for you. But I would recommend a Chiropractic evaluation to see if a chiropractic treatment regimen could be of help.
There are many approaches within chiropractic, I may be interested in a DC with spinal decompression therapy in the office if I were you. I would look for a DC with an additional credential.
At some point in the progression of your scoliosis there may be an absolute need for surgical intervention (depending upon heart lung compromise.)
Chiropractic MAY be able to improve function, decrease pain.
If you are nervous entering ANY healthcare providers office, I am with you 100%.
Looking at the facts, you may be MORE nervous in one place over another!
I hope this information helps.
I wish you good luck. Perhaps you can return to your physical therapist,perhaps they can do more work with you. Maybe the Medical Doctor has a new or different drug that can be of help.
Perhaps a surgical consult could be in order. There are many avenues to take.
YOU are the patient, it is YOUR health. Be confident and happy in the path you choose.
Please do not be upset at the statistics, I do not make the news, I only report it.
If you need further info, do not hesitate to recontact me here at:
http://allexperts.com/ep/965-100794/Chiropractors/Victor-Dolan-DC-DACBSP.htm
Thank You, Good Luck.
Dr. Victor Dolan, DC
Email NewsLetter: http://drvictordolan.chiroweb.com
References
"Death by Medicine" is an eye-opening paper published as a Web
exclusive in the March 2004 issue of Life Extension, a monthly magazine dedicated to "up-to-date coverage of the latest scientific and medical breakthroughs from around the world." As the grim title suggests, the paper explores the hazards of conventional medicine in the United States, analyzing and combining the complete published literature to date regarding injuries and deaths attributable to medicine.
1. Lazarou J, Pomeranz BH, Corey PN. Incidence of adverse drug reactions in
hospitalized patients: a meta-analysis of prospective studies. JAMA . 1998 Apr
15;279(15):1200-5.
2. Rabin R. Caution about overuse of antibiotics. Newsday . September 18, 2003
.
2a. Centers for Disease Control and Prevention. CDC antimicrobial resistance and
antibiotic resistance梘eneral information. Available at:
http://www.cdc.gov/drugresistance/community/ Accessed December 13, 2003 .
3. For calculations detail, see 揢nnecessary Surgery.?Sources: HCUPnet,
Healthcare Cost and Utilization Project. Agency for Healthcare Research and
Quality, Rockville , MD. Available at: http://www.ahrq.gov/data/hcup/hcupnet.htm
. Accessed December 18, 2003 . US Congressional House Subcommittee Oversight
Investigation. Cost and Quality of Health Care: Unnecessary Surgery . Washington
, DC : Government Printing Office;1976. Cited in: McClelland GB, Foundation for
Chiropractic Education and Research. Testimony to the Department of Veterans
Affairs' Chiropractic Advisory Committee. March 25, 2003 .
4. For calculations detail, see 揢nnecessary Hospitalization.?Sources:
HCUPnet, Healthcare Cost and Utilization Project. Agency for Healthcare Research
and Quality, Rockville , MD. Available at:
http://www.ahrq.gov/data/hcup/hcupnet.htm . Accessed December 18, 2003 . Siu AL,
Sonnenberg FA, Manning WG, et al. Inappropriate use of hospitals in a randomized
trial of health insurance plans. N Engl J Med . 1986 Nov 13;315(20):1259-66. Siu
AL, Manning WG, Benjamin B. Patient, provider and hospital characteristics
associated with inappropriate hospitalization. Am J Public Health . 1990
Oct;80(10):1253-6. Eriksen BO, Kristiansen IS, Nord E, et al. The cost of
inappropriate admissions: a study of health benefits and resource utilization in
a department of internal medicine. J Intern Med . 1999 Oct;246(4):379-87.
5. U.S. National Center for Health Statistics. National Vital Statistics Report,
vol. 51, no. 5, March 14, 2003 .
6. Thomas, EJ, Studdert DM, Burstin HR, et al. Incidence and types of adverse
events and negligent care in Utah and Colorado. Med Care. 2000 Mar;38(3):261-71.
Thomas, EJ, Studdert DM, Newhouse JP, et al. Costs of medical injuries in Utah
and Colorado . Inquiry . 1999 Fall;36(3):255-64. [Two references.]
7. Xakellis GC, Frantz R, Lewis A. Cost of pressure ulcer prevention in
long-term care. Am Geriatr Soc . 1995 May;43(5):496-501.
8. Barczak CA, Barnett RI, Childs EJ, Bosley LM. Fourth national pressure ulcer
prevalence survey. Adv Wound Care . 1997 Jul-Aug;10(4):18-26.
9. Weinstein RA. Nosocomial Infection Update. Emerg Infect Dis . 1998
Jul-Sep;4(3):416-20.
10. Fourth Decennial International Conference on Nosocomial and
Healthcare-Associated Infections. Morbidity and Mortality Weekly Report.
February 25, 2000 , Vol. 49, No. 7, p.138.
11. Burger SG, Kayser-Jones J, Bell JP. Malnutrition and dehydration in nursing
homes: key issues in prevention and treatment. National Citizens' Coalition for
Nursing Home Reform. June 2000. Available at:
http://www.cmwf.org/programs/elders/burger_mal_386.asp Accessed December 13,
2003 .
Starfield B. Is US health really the best in the world? JAMA . 2000 Jul
26;284(4):483-5. Starfield B. Deficiencies in US medical care. JAMA . 2000 Nov
1;284(17):2184-5.
HCUPnet, Healthcare Cost and Utilization Project. Agency for Healthcare Research
and Quality, Rockville , MD. Available at:
http://www.ahrq.gov/data/hcup/hcupnet.htm . Accessed December 18, 2003 .
Nationwide poll on patient safety: 100 million Americans see medical mistakes
directly touching them [press release]. McLean , VA : National Patient Safety
Foundation; October 9, 1997 .
The Society of Actuaries Health Benefit Systems Practice Advancement Committee.
The Troubled Healthcare System in the US . September 13, 2003 . Available at:
http://www.soa.org/sections/troubled_healthcare.pdf Accessed December 18, 2003
.
16. Leape LL. Error in medicine. JAMA . 1994 Dec 21;272(23):1851-7.
a.Brennan TA, Leape LL, Laird NM , et al. Incidence of adverse events and
negligence in hospitalized patients. Results of the Harvard Medical Practice
Study I. N Engl J Med . 1991 Feb 7;324(6):370-6.
Campbell EG, Weissman JS, Clarridge B, Yucel R, Causino N, Blumenthal D.
Characteristics of medical school faculty members serving on institutional
review boards: results of a national survey. Acad Med . 2003 Aug;78(8):831-6.
Possible conflict of interest within medical profession. HealthDayNews. August
15, 2003 .
20. World Health Organization. Press Release Bulletin #9. December 17, 2001 .
Angell M. Is academic medicine for sale? N Engl J Med . 2000 May
18;342(20):1516-8.
McKenzie J. Conflict of interest? Medical journal changes policy of finding
independent doctors [transcript]. ABC News. June 12, 2002 .
Crossen C. Tainted Truth: The Manipulation of Fact in America . New York , NY :
Simon & Schuster; 1994.
Bates DW, Cullen DJ, Laird N, et al. Incidence of adverse drug events and
potential adverse drug events. Implications for prevention. ADE Prevention Study
Group. JAMA . 1995 Jul 5;274(1):29-34.
Vincent C, Stanhope N, Crowley-Murphy M. Reasons for not reporting adverse
incidents: an empirical study. J Eval Clin Pract . 1999 Feb;5(1):13-21.
Wald H, Shojania KG. Incident reporting. In: Shojania KG, Duncan BW, McDonald
KM, et al, eds. Making Health Care Safer: A Critical Analysis of Patient Safety
Practices . Rockville , MD : Agency for Healthcare Research and Quality;
2001:chap 4. Evidence Report/Technology Assessment No. 43. AHRQ publication
01-E058.
Grinfeld MJ. The debate over medical error reporting. Psychiatric Times . April
2000.
King G III, Hermodson A. Peer reporting of coworker wrongdoing: A qualitative
analysis of observer attitudes in the decision to report versus not report
unethical behavior. Journal of Applied Communication Research . 2000;(28),
309-29.
Gilman AG, Rall TW, Nies AS , Taylor P. Goodman and Gilman's The Pharmacological
Basis of Therapeutics. New York , NY : Pergamon Press; 1996.
30. Kolata G. New York Times News Service. Who cares when our drugs fail? San
Diego Union-Tribune . October 15, 1997 :E-1,5.
31. Melmon KL, Morrelli HF, Hoffman BB, Nierenberg DW, eds. Melmon and
Morrelli's Clinical Pharmacology: Basic Principles in Therapeutics . 3rd ed. New
York , NY : McGraw-Hill, Inc., 1992.
Moore TJ, Psaty BM, Furberg CD. Time to act on drug safety . JAMA . 1998 May 20,
279 (19):1571-3.
32 a.Cullen DJ, Bates DW, Small SD, Cooper JB, Nemeskal AR , Leape LL. The
incident reporting system does not detect adverse drug events: a problem for
quality improvement. Jt Comm J Qual Improv . 1995 Oct;21(10):541-8.
Bates DW. Drugs and adverse drug reactions: how worried should we be? JAMA .
1998 Apr 15;279(15):1216-7.
Dickinson, JG. FDA seeks to double effort on confusing drug names. Dickinson 's
FDA Review . 2000 Mar;7(3):13-4.
Cohen JS. Overdose: The Case Against the Drug Companies . New York , NY :
Tarcher-Putnum; 2001.
Stenson J. Few residents report medical errors, survey finds. Reuters Health.
February 21, 2003 .
Survey by Henry J. Kaiser Family Foundation, Harvard School of Public Health.
Methodology: Fieldwork conducted by ICR - International Communications Research,
April 11- June 11, 2002
Bond CA, Raehl CL, Franke T. Clinical pharmacy services, hospital pharmacy
staffing, and medication errors in United States hospitals. Pharmacotherapy .
2002 Feb;22(2):134-47.
Barker KN, Flynn EA, Pepper GA, Bates DW, Mikeal RL. Medication errors observed
in 36 health care facilities. Arch Intern Med . 2002 Sep 9;162(16):1897-903.
40. LaPointe NM , Jollis JG. Medication errors in hospitalized cardiovascular
patients. Arch Intern Med . 2003 Jun 23;163(12):1461-6.
41. Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. The incidence
and severity of adverse events affecting patients after discharge from the
hospital. Ann Intern Med . 2003 Feb 4;138(3):161-7.
42. Gandhi TK, Weingart SN, Borus J, et al. Adverse drug events in
ambulatory care. N Engl J Med . 2003 Apr 17;348(16):1556-64.
43. Medication side effects strike 1 in 4. Reuters. April 17, 2003 .
44. Vastag B. Pay attention: ritalin acts much like cocaine. JAMA . 2001 Aug
22-29;286(8):905-6.
45. Rosenthal MB, Berndt ER, Donohue JM, Frank RG, Epstein AM. Promotion of
prescription drugs to consumers. N Engl J Med . 2002 Feb 14;346(7):498-505.
46. Wolfe SM. Direct-to-consumer advertising梕ducation or emotion
promotion? N Engl J Med . 2002 Feb 14;346(7):524-6.
47. Ibid.
48. US General Accounting Office. Report to the Chairman, Subcommittee on
Human Resources and Intergovernmental Relations, Committee on Government
Operations, House of Representatives: FDA Drug Review Postapproval Risks 1976-85
. Washington , DC : US General Accounting Office; 1990:3.
49. Drug giant accused of false claims. MSNBC News. July 11, 2003 .
Available at: http://msnbc.com/news/937302.asp?0sl=-42&cp1=1 Accessed December
17,2003 .
50. Suh DC , Woodall BS, Shin SK , Hermes-De Santis ER. Clinical and economic
impact of adverse drug reactions in hospitalized patients. Ann Pharmacother .
2000 Dec;34(12):1373-9.
51. Agger WA. Antibiotic resistance: unnatural selection in the office and
on the farm. Wisconsin Medical Journal . August 2002.
52. Nash DR, Harman J, Wald ER, Kelleher KJ. Antibiotic prescribing by
primary care physicians for children with upper respiratory tract infections.
Arch Pediatr Adolesc Med . 2002 Nov;156(11):1114-9.
53. Schindler C, Krappweis J, Morgenstern I, Kirch W. Prescriptions of
systemic antibiotics for children in Germany aged between 0 and 6 years.
Pharmacoepidemiol Drug Saf . 2003 Mar;12(2):113-20.
Finkelstein JA, Stille C, Nordin J, et al. Reduction in antibiotic use among US
children, 1996-2000. Pediatrics . 2003 Sep;112(3 Pt 1):620-7.
Linder JA, Stafford RS. Antibiotic treatment of adults with sore throat by
community primary care physicians: a national survey, 1989-1999. JAMA . 2001 Sep
12;286(10):1181-6.
Drug resistance page. Centers for Disease Control and Prevention website.
Available at: http://www.cdc.gov/drugresistance/community/ Accessed December
17, 2003 .
Available at: http://www.health.state.ok.us/program/cdd/ar/ Accessed December
17, 2003 .
Available at: http://www.librainitiative.com/life/en/libra_initiative.html
Accessed December 17, 2003 .
Ohlsen K, Ternes T, Werner G, et al. Impact of antibiotics on conjugational
resistance gene transfer in Staphylococcus aureus in sewage. Environ Microbiol .
2003 Aug;5(8):711-6.
60. Pawlowski S, Ternes T, Bonerz M, et al. Combined in situ and in vitro
assessment of the estrogenic activity of sewage and surface water samples.
Toxicol Sci . 2003 Sep;75(1):57-65. Epub 2003 Jun 12.
61. Ternes TA, Stuber J, Herrmann N, et al. Ozonation: a tool for removal of
pharmaceuticals, contrast media and musk fragrances from wastewater? Water Res .
2003 Apr;37(8):1976-82.
62. Ternes TA, Meisenheimer M, McDowell D, et al. Removal of pharmaceuticals
during drinking water treatment. Environ Sci Technol . 2002 Sep
1;36(17):3855-63.
63. Ternes T, Bonerz M, Schmidt T. Determination of neutral pharmaceuticals
in wastewater and rivers by liquid chromatography-electrospray tandem mass
spectrometry. J Chromatogr A . 2001 Dec 14;938(1-2):175-85.
64. Golet EM, Alder AC, Hartmann A, Ternes TA, Giger W. Trace determination
of fluoroquinolone antibacterial agents in urban wastewater by solid-phase
extraction and liquid chromatography with fluorescence detection. Anal Chem .
2001 Aug 1;73(15):3632-8.
65. Daughton CG, Ternes TA. Pharmaceuticals and personal care products in
the environment: agents of subtle change? Environ Health Perspect . 1999 Dec;107
Suppl 6:907-38.
66. Hirsch R, Ternes T, Haberer K, Kratz KL. Occurrence of antibiotics in
the aquatic environment. Sci Total Environ . 1999 Jan 12;225(1-2):109-18.
67. Ternes TA, Stumpf M, Mueller J, Haberer K, Wilken RD , Servos M.
Behavior and occurrence of estrogens in municipal sewage treatment plants桰.
Investigations in Germany , Canada and Brazil . Sci Total Environ . 1999 Jan
12;225(1-2):81-90.
68. Hirsch R, Ternes TA, Haberer K, Mehlich A, Ballwanz F, Kratz KL.
Determination of antibiotics in different water compartments via liquid
chromatography-electrospray tandem mass spectrometry. J Chromatogr A . 1998 Jul
31;815(2):213-23.
69. Coste J, Hanotin C, Leutenegger E. Prescription of non-steroidal
anti-inflammatory agents and risk of iatrogenic adverse effects: a survey of
1072 French general practitioners. Therapie . 1995 May-Jun;50(3):265-70.
70. Kouyanou K, Pither CE, Wessely S. Iatrogenic factors and chronic pain.
Psychosom Med . 1997 Nov-Dec;59(6):597-604.
Abel U. Chemotherapy of advanced epithelial cancer梐 critical review. Biomed
Pharmacother . 1992;46(10):439-52.
Schulman KA, Stadtmauer EA, Reed SD , et al. Economic analysis of
conventional-dose chemotherapy compared with high-dose chemotherapy plus
autologous hematopoietic stem-cell transplantation for metastatic breast cancer.
Bone Marrow Transplant . 2003 Feb;31(3):205-10.
Kaufman, M. Drugmaker to pay FDA $500 million. Manufacturing problems found at
schering-plough . The Washington Post . May 18, 2002 :A01.
US Congressional House Subcommittee Oversight Investigation. Cost and Quality of
Health Care: Unnecessary Surgery . Washington , DC : Government Printing
Office;1976. Cited in: McClelland GB, Foundation for Chiropractic Education and
Research. Testimony to the Department of Veterans Affairs' Chiropractic Advisory
Committee. March 25, 2003 .
75. Leape LL. Unnecessary surgery. Health Serv Res . 1989 Aug;24(3):351-407.
76. McClelland GB, Foundation for Chiropractic Education and Research.
Testimony to the Department of Veterans Affairs' Chiropractic Advisory
Committee. March 25, 2003 .
77. Coile RC Jr. Internet-driven surgery. Russ Coiles Health Trends . 2003
Jun;15(8):2-4.
78. Guarner V. Unnecessary operations in the exercise of surgery. A topic of
our times with serious implications in medical ethics. Gac Med Mex . 2000
Mar-Apr;136(2):183-8.
79. Rutkow IM. Surgical operations in the United States : 1979 to 1984.
Surgery . 1987 Feb;101(2):192-200.
80. Rutkow IM. Surgical operations in the United States . Then (1983) and now
(1994). Arch Surg . 1997 Sep;132(9):983-90.
81. Linnemann MU, Bulow HH. Infections after insertion of epidural catheters.
Ugeskr Laeger . 1993 Jul 26;155(30):2350-2
Seres JL, Newman RI . Perspectives on surgical indications. Implications for
controls. Clin J Pain . 1989 Jun;5(2):131-6.
Chassin MR, Kosecoff J, Park RE, et al. Does inappropriate use explain
geographic variations in the use of health care services? A study of three
procedures. JAMA. 1987 Nov 13;258(18):2533-7.
84. Office of Technology Assessment, US Congress. Assessing the Efficacy and
Safety of Medical Technologies. Washington DC : Office of Technology Assessment,
US Congress; 1978.
85. Tunis SR, Gelband H. Health care technology in the United States .
Health Policy . 1994 Oct-Dec;30(1-3):335-96.
Zhan C, Miller M. Excess length of stay, charges, and mortality attributable to
medical injuries during hospitalization. JAMA . 2003;290:1868-1874.
Injuries in hospitals pose a significant threat to patients and a substantial
increase in health care charges [press release]. Rockville , MD : Agency for
Healthcare Research and Quality. October 7, 2003 .
http://www.ahrq.gov/news/ress/pr2003/injurypr.htm
Weingart SN, Iezzoni LI. Looking for medical injuries where the light is bright.
JAMA . 2003 Oct 8 ;290(14):1917-9.
MacMahon B. Prenatal x-ray exposure and childhood cancer. J Natl Cancer Inst .
1962 May;28:1173-91.
90. Health Physics Society. Available at:
http://hps.org/publicinformation/ate/q1084.html Accessed December 17, 2003 .
Gofman JW. Radiation from Medical Procedures in the Pathogenesis of Cancer and
Ischemic Heart Disease: Dose-Response Studies with Physicians per 100,000
Population. San Francisco , CA : CNR Books; 1999.
Gofman J W. Preventing Breast Cancer: The Story of a Major, Proven, Preventable
Cause of This Disease . 2nd ed. San Francisco , CA : CNR Books; 1996.
Sarno JE. Healing Back Pain: The Mind-Body Connection . Warner Books; 1991.
Siu AL, Sonnenberg FA, Manning WG, et al. Inappropriate use of hospitals in a
randomized trial of health insurance plans. N Engl J Med . 1986 Nov
13;315(20):1259-66.
95. Siu AL, Manning WG, Benjamin B. Patient, provider and hospital
characteristics associated with inappropriate hospitalization. Am J Public
Health . 1990 Oct;80(10):1253-6.
Eriksen BO, Kristiansen IS, Nord E, et al. The cost of inappropriate admissions:
a study of health benefits and resource utilization in a department of internal
medicine. J Intern Med . 1999 Oct;246(4):379-87.
Showalter E. Hystories: Hysterical Epidemics and Modern Media . New York , NY :
Columbia University Press; 1997.
Fugh-Berman A. Alternative healing. In: Smith B, Steinem G, Mink G, Navarro M,
and Mankiller W, eds. The Reader's Companion to U.S. Women's History. New York ,
NY : Houghton Mifflin; 1998. Available at:
http://college.hmco.com/history/readerscomp/women/html/wh_001200_alternativeh.ht...
.
Thacker SB, Stroup D, Chang M. Continuous electronic heart rate monitoring for
fetal assessment during labor (Cochrane Review). In: The Cochrane Library, issue
1, 2003. Oxford : Update Software.
100. Cole C. Admission electronic fetal monitoring does not improve neonatal
outcomes . J Fam Pract . 2003 Jun;52(6):443-4.
101. Nelson HD, Humphrey LI, Nygren P, Teutsch SM, Allan JD. Postmenopausal
hormone replacement therapy: scientific review. JAMA . 2002 Aug
21;288(7):872?1.
102. Nelson HD. Assessing benefits and harms of hormone replacement therapy:
clinical applications. JAMA . 2002 Aug 21;288(7):882-4
103. Fletcher SW, Colditz GA. Failure of estrogen plus progestin therapy for
prevention. JAMA . 2002 Jul 17;288(3):366-8.
104. Rossouw JE, Anderson GL, Prentice RL, et al; Writing Group for the
Women's Health Initiative Investigators. Risks and benefits of estrogen plus
progestin in healthy postmenopausal women: principal results from the Women's
Health Initiative randomized controlled trial. JAMA . 2002 Jul 17;288(3):321-33.
105. Rutkow IM. Obstetric and gynecologic operations in the United States ,
1979 to 1984. Obstet Gynecol . 1986 Jun;67(6):755-9.
106. Family Practice News . February 15, 1995 : 29.
Sakala C. Medically unnecessary cesarean section births: introduction to a
symposium. Soc Sci Med . 1993 Nov;37(10):1177-98.
VanHam MA, van Dongen PW, Mulder J. Maternal consequences of cesarean section. A
retrospective study of intra-operative and postoperative maternal complications
of cesarean section during a 10-year period. Eur J Obstet Reprod Biol . 1997
Jul;74(1):1-6.
Weiner J. Smoking and cancer: the cigarette papers: how the industry is trying
to smoke us all . The Nation . January 1, 1996 :11-18.
110. Tobacco.org. Tobacco timeline. Available at:
http://www.tobacco.org/resources/history/tobacco_history.html Acccessed
December 16, 2003 .
111. Lasser KE, Allen PD, Woolhandler SJ, Himmelstein DU, Wolfe SM, Bor DH.
2002. Timing of new black box warnings and withdrawals for prescription
medications. JAMA . 2002 May 1;287(17):2215-20.
112. Injuryboard.com. General Accounting Office study sheds light on nursing
home abuse. July 17, 2003 . Available at:
http://www.injuryboard.com/view.cfm/Article=3005 Accessed December 17, 2003 .
113. Weingart SN, McL Wilson R, Gibberd RW, Harrison B. Epidemiology of
medical error. West J Med . 2000 Jun;172(6):390-3.
114. Blendon R, Schoen C, et al. Five nation survey exposes flaws in the U.S.
health care system. Health Affairs . May/June 2002.
115. Institute of Medicine . Care Without Coverage: Too Little, Too Late .
May 21, 2002 . A Shared Destiny: Community Effects of Uninsurance . March 6,
2003 .
US Department of Health and Human Services and US Department of Justice. Health
Care Fraud and Abuse Control Program Annual Report for FY 1998. April 1999.
Health Care Fraud and Abuse Control Program Annual Report for FY 2001. April
2002.
Abuse of residents is a major problem in U.S. nursing homes [transcript]. CNN
television. July 30, 2001
117 a. Available at: http://www.house.gov/waxman Accessed December 17, 2003 .
Mitka M. Unacceptable nursing home deaths unautopsied. JAMA . 1998 Sep
23-30;280(12):1038-9
New data is in on North Carolina 's nursing home residents. Medical Review of
North Carolina, Inc. July 21, 2003 .
120. Weinstein RA. Nosocomial infection update. Emerg Infect Dis . 1998
Jul-Sep;4(3):416-20.
Centers for Medicare & Medicaid Services. Report to Congress: Appropriateness of
Minimum Nurse Staffing Ratios In Nursing Homes: Phase II Final Report . December
24, 2001 .
Consumer group criticizes Thompson letter dismissing report on dangerous
staffing levels in nursing homes [news release]. Washington , DC : National
Citizens' Coalition for Nursing Home Reform. March 22, 2002 .
Bergstrom N, Braden B, Kemp M, Champagne M, Ruby E. Multi-site study of
incidence of pressure ulcers and the relationship between risk level,
demographic characteristics, diagnoses and prescription of preventive
interventions . J Am Geriatr Soc . 1996 Jan;44(1):22-30.
Miles SH. Concealing accidental nursing home deaths. HEC Forum . 2002
Sep;14(3):224-34.
Corey TS, Weakley-Jones B, Nichols GR 2nd, Theuer HH. Unnatural deaths in
nursing home patients. J Forensic Sci . 1992 Jan;37(1):222-7.
Lloyd-Jones DM, Martin DO, Larson MG, Levy D. Accuracy of death certificates for
coding coronary heart disease as the cause of death. Ann Intern Med . 1998 Dec
15;129(12):1020-6.
Thomas DR , Zdrowski CD, Wilson MM, et al. Malnutrition in subacute care. Am J
Clin Nutr . 2002 Feb;75(2):308-13.
Robinson BE. Death by destruction of will. Lest we forget. Arch Intern Med .
1995 Nov 13;155(20):2250-1.
Capezuti E, Strumpf NE, Evans LK, Grisso JA, Maislin G. The relationship between
physical restraint removal and falls and injuries among nursing home residents .
J Gerontol A Biol Sci Med Sci . 1998 Jan;53(1):M47-52.
130. Phillips CD, Hawes C, Fries BE. Reducing the use of physical
restraints in nursing homes: will it increase costs? Am J Public Health . 1993
Mar;83(3):342-8.
Miles SH, Irvine P. Deaths caused by physical restraints. Gerontologist . 1992
Dec;32(6):762-6.
Annas GJ. The last resort梩he use of physical restraints in medical
emergencies. N Engl J Med . 1999 Oct 28;341(18):1408-12.
Parker K, Miles SH. Deaths caused by bedrails. J Am Geriatr Soc . 1997
Jul;45(7):797-802.
Miles SH. Concealing accidental nursing home deaths. HEC Forum . 2002
Sep;14(3):224-34.
Katz PR, Seidel G. Nursing home autopsies. Survey of physician attitudes and
practice patterns. Arch Pathol Lab Med . 1990 Feb;114(2):145-7.
Overmedication of U.S. seniors. Reuters Health. May 21, 2003 .
Average number of prescriptions by HMOs increases. Drug Benefit Trends . 2002
Sep 12;14(8).
Kaiser Family Foundation. Prescription Drug Trends . November 2001.
Williams BR, Nichol MB, Lowe B, Yoon PS, McCombs JS, Margolies J. Medication use
in residential care facilities for the elderly. Ann Pharmacother . 1999
Feb;33(2):149-55.
140. AARP. Medicare and prescription drugs. Available at:
http://www.aarp.org/prescriptiondrugs Accessed December 16, 2003 .
California reaches $100 million multi-state settlement with drug giant Mylan
over alleged price-fixing scheme [press release]. Sacramento , CA : Office of
the Attorney General, Department of Justice, State of California ; July 12, 2000
.
Attorney general reaches settlement with drug giant. WRAL News. March 7, 2003 .
Available at: . http://www.wral.com/money/2026364/detail.html . Accessed
December 16, 2003 .
Blowing the final whistle. The Observer. November 25, 2001 . Available at:
http://education.guardian.co.uk/businessofresearch/comment/0,9976,606260,00.html
Accessed December 16, 2003 .
AARP. Are food supplements for me. Available at:
http://www.aarp.org/Articles/a2003-03-07-supplements.html Accessed December
16,2003 .
145. Bernabei R, Gambassi G, Lapane K, et al. Management of pain in elderly
patients with cancer. SAGE study group. Systematic assessment of geriatric drug
use via epidemiology. JAMA . 1998 Jun 17;279(23):1877-82.
Associated Press. Panel names estrogen as carcinogen. The Washington Post .
December 16, 2000 :A05.
Estrogen hikes ovarian cancer risk. MSNBC staff and wire reports. July 16, 2002
. Grady D. Study recommends NOT using hormone therapy for bone loss. New York
Times . October 1, 2003 .
Anderson GL, Judd HL, Kaunitz AM, et al. Effects of estrogen plus progestin on
gynecologic cancers and associated diagnostic procedures: the Women's Health
Initiative randomized trial. JAMA . 2003 Oct 1;290(13):1739-48.
Chlebowski RT, Hendrix SL, Langer RD , et al. Influence of estrogen plus
progestin on breast cancer and mammography in healthy postmenopausal women: the
Women's Health Initiative randomized trial. JAMA . 2003 Jun 25;289(24):3243-53.
150. Wassertheil-Smoller S, Hendrix SL, Limacher M, et al . Effect of
estrogen plus progestin on stroke in postmenopausal women: the Women's Health
Initiative: a randomized trial. JAMA . 2003 May 28;289(20):2673-84.
151. Shumaker SA, Legault C, Rapp SR, et al. Estrogen plus progestin and the
incidence of dementia and mild cognitive impairment in postmenopausal women: the
Women's Health Initiative memory study: a randomized controlled trial. JAMA
2003;289:2651-62 .
152. Beral V; Million Women Study Collaborators. Breast cancer and
hormone-replacement therapy in the Million Women Study. Lancet . 2003 Aug
9;362(9382):419-27.