Since the introduction of the low-friction total hip arthroplasty (THA) by Sir John Charnley,[1, 2, 3, 4] wear has been a primary issue in hip arthroplasty. Charnley's original choice for bearing surfaces was a stainless-steel head on polytetrafluoroethylene (PTFE). This choice was complicated by a wear rate of 7-10 mm within a 3-year period. This led him to search for other bearing materials, namely high-molecular-weight polyethylene. Although wear remains a problematic issue in THA, its consequences—namely, osteolysis and prosthetic loosening—loom as larger issues.
Wear results when surfaces produce local mechanical damage and unwanted loss of material and the resultant generation of wear particles. Conventional wear includes fatigue and interfacial (bearing surface) wear. Fatigue wear occurs as a result of repetitive stressing of a bearing material. Interfacial wear is divided into abrasive and adhesive wear.
Abrasive wear occurs when a surface asperity cuts or plows into the opposing surface. This may be especially true when the two surface materials have different hardnesses and the harder material cuts into the softer material. Adhesive wear occurs when bonding of microcontacts exceeds the inherent strength of either material. The weaker material may then be torn off and adhere to the stronger material. Other factors in wear include surface roughness, material hardness, contact areas, and loads applied.[5, 6, 7, 8, 9, 10, 11, 12, 13]
For patient education resources, see Total Hip Replacement.
NextThe relevant anatomy is that of the hip, acetabulum, pelvis, and proximal femur. Surgeons dealing with the complications of acetabular wear in THA must be familiar with the anatomy of the region. In addition, they should be comfortable with a variety of extensile surgical approaches. The armamentarium of surgical approaches includes the following:
The most frequently used surgical approaches are the direct lateral, anterolateral, and posterior approaches. Commonly used modifications to the most frequently used approaches include the trochanteric slide, the trochanteric osteotomy, and the extended trochanteric osteotomy.
Willert found that capsular tissue has some capacity to transport wear particles through the lymphatic system by way of perivascular lymph spaces.[14] If this system is overwhelmed, then these particles accumulate in periarticular tissues and are subsequently phagocytosed by macrophages in the pseudocapsule. This process results in foreign body granuloma formation with areas of necrosis and fibrosis. Extension of this foreign body response may infiltrate into the cement-bone or bone-implant interface and may result in loosening.
Polyethylene particles disperse into the joint fluid surrounding a THA. The effective joint space includes all periprosthetic regions accessible to joint fluid and thereby accessible to particulate wear debris. The quality of contact within the implant-bone, cement-bone, or implant-cement interface determines the limits of the effective joint space. Much variability exists in these contacts for each reconstruction. Joint fluid flows according to pressure gradients and follows the path of least resistance. These patterns shape the extent of osteolysis. Finally, the effective joint space can also expand into soft tissues as well as bone.
Stress shielding may result in periprosthetic bone loss from a reduction in the load transmitted to bone. Periprosthetic bone loss may also occur as a result of an inflammatory reaction due to particulate wear debris as generated in the various wear modes (see Presentation, Modes of Wear).
Tissues adjacent to hip replacements consist of synovial and fibrous tissue, lymphocytes, and foreign body inflammatory cells. The number of foreign body inflammatory cells (macrophages and giant cells) present correlates with the number of polyethylene wear particles. Wear particles produce a series of responses on both cellular and tissue levels.
The macrophage appears to be central in the biologic response to wear debris. Macrophages phagocytose small wear particles and may fuse to form foreign body giant cells. Osteoclasts are responsible for most periprosthetic bone resorption. Some evidence also suggests that macrophages and foreign body giant cells may also be capable of direct low-grade resorption.
Activated macrophages release cytokines (interleukins and prostaglandins) that are responsible for the recruitment and differentiation of cells and may also stimulate bone resorption. Macrophages release both interleukin (IL)-1β and tumor necrosis factor (TNF). Matrix metalloproteinases (MMPs) are produced by interfacial membrane tissues around hip replacements and can also affect bone resorption.
The in-vitro response of macrophages to wear debris is a function of the size, shape, and composition of particles. The macrophage response is also dose-dependent. The size of the particles is also important in their ability to stimulate an inflammatory response. Particles larger than 7 µm and smaller than 0.2 µm have less stimulatory effect than those within that range.
Osteolysis has typically been described as nonlinear, scalloped, or erosive femoral endosteal bone resorption associated with cemented hip prostheses. Osteolysis clearly is bone resorption in association with foreign body response to wear particles.
Charnley reported nonlinear endosteal erosions in association with cemented Charnley THA. He incorrectly suspected that this bone loss was due to infection. He also noted cystic erosions in the femoral diaphysis in association with stem fracture and related this finding to a deficient cement mantle. Periprosthetic tissues were noted to contain cement particles, though polyethylene particles were not found.[15]
Harris noted a similar pattern of localized bone resorption around a loose THA.[16] These tissues were found to have a high degree of osteoclastic bone resorption, a high concentration of macrophages, and occasional foreign body giant cells with phagocytosed cement particles, leading to what was called cement disease. Jasty also noted osteolysis in association with well-fixed components with adjacent cement particles.[17] Polyethylene particles were not implicated as the cause of osteolysis until cementless components were inserted and subsequently shown to have endosteal osteolysis.
Anthony demonstrated a communication between the bearing surface articulation and the endosteal surface of the femur.[18] This communication was through a space between the stem and the cement and then through a defect in the cement mantle. Particles of cement, metal, and polyethylene were found in macrophages in these osteolytic lesions. Arthrography confirmed the transfer of contrast material from the articulation to the areas of osteolysis. A common finding in patients with osteolysis around a cemented component is a defect in the cement mantle. The risk of osteolysis may be decreased if technical errors are minimized.
Cementless femoral components with limited proximal porous coatings have been associated with localized bone resorption in the diaphysis. This appears to be due to the limited proximal porous coating, especially if it is not circumferential, which allows egress of joint fluid laden with wear debris and access to the diaphyseal endosteum. Circumferential extensively coated stems have not been associated with diaphyseal osteolysis, even in the presence of proximal stress shielding. (See the images below.)
 Acetabular wear in total hip arthroplasty. Cementless total hip arthroplasty in a 60-year-old woman with osteoarthritis.
Acetabular wear in total hip arthroplasty. Cementless total hip arthroplasty in a 60-year-old woman with osteoarthritis.
 Acetabular wear in total hip arthroplasty. Woman who underwent cementless total hip arthroplasty for osteoarthritis at age 60 years, 6 years following the index arthroplasty. This image demonstrates eccentric polyethylene wear, osteolysis, and a protrusio defect. The stem appears to be well fixed.
Acetabular wear in total hip arthroplasty. Woman who underwent cementless total hip arthroplasty for osteoarthritis at age 60 years, 6 years following the index arthroplasty. This image demonstrates eccentric polyethylene wear, osteolysis, and a protrusio defect. The stem appears to be well fixed.
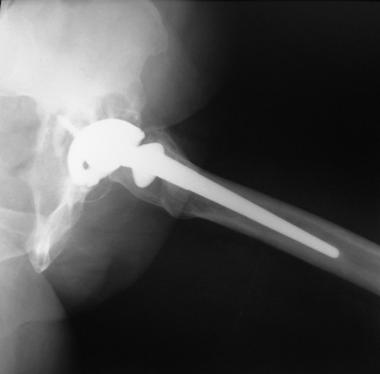 Acetabular wear in total hip arthroplasty. Lateral radiograph of the left hip of woman who underwent cementless total hip arthroplasty for osteoarthritis at age 60 years, 6 years following the index arthroplasty. She has eccentric polyethylene wear, osteolysis, and a protrusio defect. The stem is well fixed.
Acetabular wear in total hip arthroplasty. Lateral radiograph of the left hip of woman who underwent cementless total hip arthroplasty for osteoarthritis at age 60 years, 6 years following the index arthroplasty. She has eccentric polyethylene wear, osteolysis, and a protrusio defect. The stem is well fixed.
Osteolysis can occur in a more linear pattern and progress along a bone-cement interface and contribute to implant loosening. This is especially true for cemented acetabular components. Once stability is lost, further motion can only be detrimental. A highly significant association has been demonstrated between the rate of polyethylene wear and loosening of an acetabular component. Cementless acetabular components may also be subjected to a similar process of linear osteolysis. The integrity of the implant bone interface governs the ingress of joint fluid and wear particles. Acetabular components with tight peripheral press fit reduce the prevalence of progressive peripheral interface radiolucencies.
Cementless acetabular components appear to have a lower prevalence of interface radiolucencies than cemented acetabular components do. Bone resorption associated with cemented acetabular components occurs predominantly along the interface and follows the edge of the cement mantle. Bone resorption in cementless acetabular components progresses away from the interface and into the cancellous bone of the pelvis, resulting in nonlinear osteolysis or expansile osteolysis.
Pelvic osteolysis is associated with younger patients, vertical component positioning, and high volumetric wear of the polyethylene. Other concerns regarding cementless acetabular components are wear of the convex surface of the modular polyethylene insert (backside wear) and fretting of the fixation screws placed into the shell. Backside wear may be especially prominent in acetabular shell designs with poor locking mechanisms that allow significant motion between the polyethylene liner and the concave surface of the acetabular shell.
A randomized controlled trial evaluated the results of component fixation with and without cement. Using data from 250 patients with osteoarthritis (mean age, 64 years) who were treated with total hip arthroplasty, the authors found significantly lower survival rates for cemented implants compared with cementless implants after a minimum of 17 years of follow-up.[19]
In the 1990s, submicron polyethylene wear particles were recognized as being produced in very large numbers, even by well-functioning prostheses. The concentration of wear particles can extend into the billions per gram of tissue in periprosthetic areas. Wear particles are a function of the type of wear that produces them.
In-vivo wear assessments have traditionally been based on radiography. The degree of penetration of the femoral component into the polyethylene on sequential radiography has been noted as linear wear. The method of radiographic assessment most commonly used is a technique described by Livermore.[20]
On sequential radiography, the distance from the center of the femoral head to a particular reference point on the acetabular cup is measured and corrected for magnification. The difference from the initial postoperative radiograph to the most recent radiograph represents linear wear as measured in millimeters. The linear wear rate is that measurement over the period of implantation. The difficulty with this technique for evaluating linear wear is that it cannot distinguish linear wear from creep or plastic deformation.
Perhaps linear wear would more accurately be termed linear penetration. Creep is most notable early in the postoperative period and becomes negligible after 12-18 months. Additionally, backside or mode 4 wear could also contribute to higher rates of linear penetration.
Volumetric wear is a measure of the volume of material removed from a bearing surface. Computer-assisted techniques with digitized radiography have been used with reasonable reliability. Other techniques have included the shadowgraph technique and fluid-displacement methods for retrieved specimens.
Many variables affect in-vivo wear; as a result, reports regarding wear rates have shown great variability. Patient variables include age, sex, weight, general health, and activity level. Variables related to the hip reconstruction include the choice of bearing material, the design and manufacturing of the prosthesis, and characteristics of implantation (ie, operative technique, biomechanical considerations, initial and long-term implant fixation). Multiple assessments of wear over time are more valuable than a single measurement, and comparing rates of linear penetration after different durations of implantation may be difficult.
Both theoretical models and retrieval analyses have shown that the rates of volumetric wear in polyethylene components increases with increases in the diameter of the femoral head. Using a simple cylindrical formula in which volume equals π multiplied by the radius squared, for any given amount of linear wear, the volumetric wear increases exponentially with increases in the femoral head. Findings of a retrieval study showed that for each 1-mm increase in head diameter, volumetric wear increased by 6.3 mm3/y. Similarly, the rate of volumetric wear increased from 7.5% to 10% for each 1-mm increase in head diameter.
In-vivo studies comparing 32-mm heads with smaller heads have shown similar or greater wear rates. Larger heads have also been associated with bone resorption and loosening. Because of their large diameters, surface replacement components have rates of volumetric polyethylene wear four to 10 times higher than conventional THA with 28-mm heads. One potential benefit of larger heads was thought to be a reduction in polyethylene stresses because of large contact areas and thereby a reduction in linear wear. This, however, has not been the case. Thin polyethylene in some 32-mm bearings and in surface replacements has also confounded the relation between wear and the diameter of the femoral head.
The association between volumetric wear and periprosthetic bone resorption appears to be related to the volume of polyethylene wear particles created. Studies of wear particles from retrieved periprosthetic tissues and worn polyethylene surfaces are consistent with an average particle size in the range of 0.5 µm in diameter. A 28-mm head with linear wear of 0.05 mm/y corresponds to a volumetric wear rate of 30 mm3/y. This would also correlate with 500 billion particles, given an average particle diameter of 0.5 µm.
Schmalzried noted a 45-fold difference in the range of gait cycles from the least active to the most active individual.[7] Variation in an individual's activity contributes to the variability in wear rates that are commonly observed in in-vivo studies.
The outcome and prognosis are related to the surgical procedure performed and mirror experiences with revision hip arthroplasty. Prognosis may be further influenced by implant materials and designs and by potential surgical complications.
Clinical Presentation
Copyright © www.orthopaedics.win Bone Health All Rights Reserved