Patella is commonly referred to as the kneecap. This Buzzle article provides everything you need to know about patella alta, which is a rare condition wherein the kneecap is positioned higher than usual.
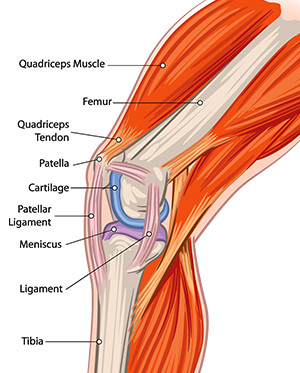
Did You Know?Patella fractures, which could occur in the event of direct or indirect trauma, account for almost 1% of all fractures.The largest joint of the human body, the knee is formed by articulations between three bones called femur (thigh bone), patella (kneecap), and tibia (one of the lower leg bones). While the medial and lateral condyles of the thigh bone articulate with tibia, the anterior (front) and distal part of the thigh bone articulates with patella. The kneecap is a small, triangular-shaped bone that rests between the femur and tibia, and slides along in the groove of the thigh bone. It is categorized as a sesamoid bone, which refers to a bone that is embedded within a tendon. Patella is embedded within the tendon of the quadriceps femoris. If patella or the quadriceps tendon gets inflamed or damaged, the affected individual is likely to experience pain or difficulty while bending the leg or performing leg movements such as walking, standing, running, jumping, etc.
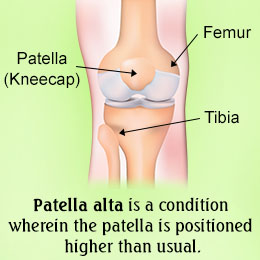
Dislocation and subluxation (incomplete dislocation) of the patella can occur in case of trauma, or in case of individuals affected by a condition called patella alta, wherein the kneecap (patella) is positioned higher than usual in relation to the thigh bone. Attenuated patella alta is characterized by an unusually small kneecap. On the other hand, patella baja or infera, is a condition that is characterized by an abnormally low patella.
Patella and Knee Stability
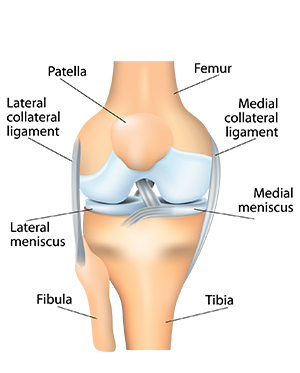
Patella is important for the stability of the knee joint. Under normal circumstances, the kneecap and the thigh bone (bones of the PFJ or patellofemoral joint) move smoothly against one another when the knee is flexed or extended. During such movements, the kneecap glides in the trochlear groove or sulcus in the thigh bone. Moreover, tendons, soft tissues, and ligaments also provide support and stability to the knee joint. In case of people with a thin built and tall stature, the kneecap might lie above the trochlear groove, resulting in patella alta.
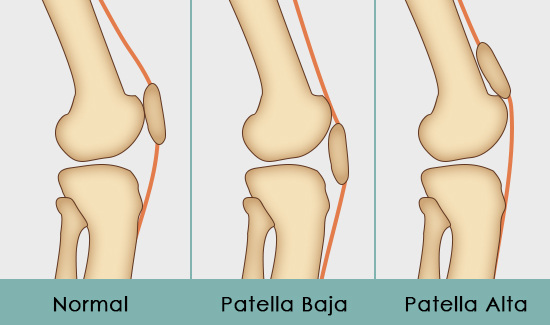
Also referred to as a high-ride kneecap, patella alta is quite rare. It must be noted that this condition could be present at birth. It could occur when the tendon that connects the kneecap to the tibia (shinbone) is longer than normal. This condition could occur in the event of trauma (rupturing of the patellar tendon) or complication of a surgery. It could give rise to the following symptoms:
➠ Anterior knee pain (pain in the front section of the knee)
➠ Instability of the kneecap
➠ Unsteady gait
➠ Adverse effect on the mobility of the knee
➠ Increased risk of subluxation or dislocation
This condition could be associated with Osgood-Schlatter's disease. It is believed that this condition could put one at a risk of developing patellofemoral pain. It is also associated with recurrent dislocation of the patella, chondromalacia patellae (softening and degeneration of the articular hyaline cartilage of the patella), and joint effusion (fluid buildup in a joint). Therefore, attention must be paid to the position of the patella in case of individuals who have been complaining about anterior knee pain.
In a study conducted by Ward et al., it was found that the individuals affected with patella alta were at a greater risk of developing malalignment of PFJ, decreased PFJ contact area, and increased stress on the joint. Thus, this condition could make one susceptible to damage to the cartilage and underlying bone in the patellofemoral joint.
Determination of Patellar Height
Usually, lateral knee X-rays that are conducted with the knee flexed at 20-30°, help in the determination of the height of the kneecap. The degree of knee flexion is important, as it provides the right tension of the patellar tendon, which helps in calculating the height. Though numerous methods have been presented for calculating the patellar height in relation to the tibiofemoral joint and determining if the kneecap is positioned higher or lower than usual, these methods come with their own set of advantages and disadvantages. Methods have been described by Insall and Salvati, Blackburne and Peel, Caton et al., deCarvalho et al., Micheli et al., Egund et al., Koshino and Sugimoto, Grelsamer and Meadows (Modified Insall and Salvati method), and Leung et al. Out of these, the following methods are commonly used for determining the height of the kneecap:
➠ Insall and Salvati method
➠ Blackburne and Peel method
➠ Modified Insall-Salvati method
➠ Caton-Deschamps method
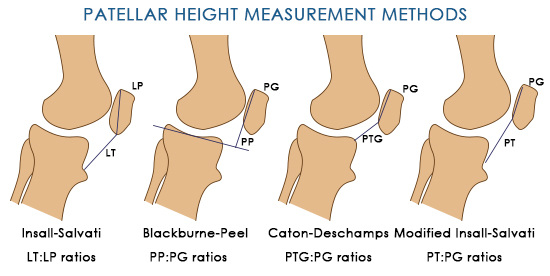
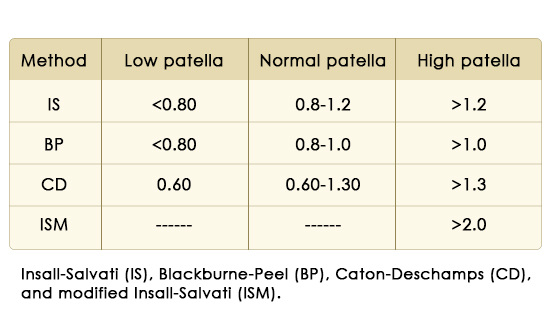
In case of Insall and Salvati method, the length of the patellar tendon and the length of patella is measured with the help of lateral radiograph of the knee, with the knees flexed at an angle between 20° and 70° (usually 30°). While the length of the patellar tendon is obtained by measuring the length of the inner border of the patellar tendon from the lower pole of the patella to the notch in the tibial cortex at the superior border of the tibial tubercle, the length of the patella is measured as an oblique line connecting the inner margin of the upper pole of the patella with the most inferior point of the lower pole. Normally, the ratio of the length of patellar tendon and the length of patella should be within the range of 0.8 to 1.2. If the ratio is higher than 1.2, it is indicative of patella alta.
In case of the Blackburne and Peel method, a lateral radiograph of the knee with 30 degrees of flexion is obtained and the ratio of the articular surface length of the patella to the height of the lower pole of the articular surface above a tibial plateau line (ratio between the perpendicular distance from lower articular margin of patella to tibial plateau and the length of articular surface of patella) is measured. If the ratio is greater than 1, it is indicative of patella alta.
In case of the modified Insall and Salvati method, the length of the patellar tendon is divided by the length of the articular surface of the patella (PC). This method was suggested, taking into consideration the variability in the shape of the lower pole of the patella.
Caton-Deschamps index refers to the ratio between the distance between upper part of tibia and inferior part of patella (a) and the length of articular surface of patella (b). If a/b value is greater than 1.2, it is indicative of patella alta.
Treatment
Since the symptoms can worsen in case of repeated stress to the joint, people affected by this condition should take ample rest to get relief from pain. Moreover, taking rest from strenuous physical activities involving the knee joint will reduce stress on the patella and help restore strength and stability of the knee joint. The RICE (Rest, Ice, Compression, and Elevation) approach might prove to be beneficial. While rest reduces the stress on the kneecap, the application of ice and compression (wrapping the affected area) would help reduce the swelling. Elevating the area above the level of the heart while sitting or lying down also minimizes the swelling. Physical therapy is also an essential part of the treatment. Exercises can help in strengthening the joint.
The patient will have to undergo a surgical procedure in severe cases, when conservative treatment doesn't work. In some cases, patella alta treatment can include surgical procedures such as patellectomy, tibial tuberosity advancement osteotomy, or arthroscopic lateral release. First of all, the condition and position of the patella is evaluated with the help of arthroscopy. Thereafter, open or arthroscopic surgical procedures might be recommended to correct the problem.
In case of tibial tuberosity advancement osteotomy, an incision is made at the front of the knee, directly over the tibial tuberosity, and the tibial tuberosity (with the patellar tendon) is cut from the front of the tibia and shifted downwards. This is followed by the placement of the bone of the tibial tuberosity into place in the new position with the help of a screw and a steel wire band.
In case of lateral release, the tight ligaments on the lateral side of the kneecap are cut. This allows it to slide more towards the center of the groove of the thigh bone. Over time, the ligaments would heal and the gap created by this surgical procedure would be filled by the scar tissue. Thus, the patella is shifted back to the normal position and pressure on the articular cartilage is relieved. However, this procedure is not considered to be a very effective treatment option for patellar instability. In rare cases, the partial/complete removal of the kneecap might be recommended.
On a concluding note, an abnormally high kneecap can cause a host of symptoms and make one susceptible to the dislocation of the kneecap. Thus, medical assistance must be sought by those who are affected by this condition. It must be noted that habitual dislocation (some individuals who have a habit of dislocating their kneecap at will) must be avoided at all costs. Though this habit might seem to be harmless, it can put one at a risk of developing osteoarthritis.
Disclaimer:
The information provided in this article is solely for educating the reader. It is not intended to be a substitute for the advice of a medical expert.