Rheumatoid arthritis (RA) is a progressive, systemic, autoimmune disease that causes joint inflammation. At onset, small joints such as the hands, wrists, and feet tend to be involved more than large joints. Because it is a systemic disease RA can cause significant internal organ damage to areas such as the lungs, skin, blood-producing organs, heart, and eyes.
More than 2 million Americans are affected by RA.
It is critical to make the diagnosis of RA as quickly as possible in order to prevent damage to both joints as well as internal organs.
The traditional criteria for establishing the diagnosis of rheumatoid arthritis are the American College of Rheumatology criteria:
1.Morning stiffness in and around joints, lasting at least I hour before maximal improvement.
2.Arthritis of 3 or more joint areas simultaneously with soft tissue swelling observed by a physician. The possible areas include the fingers, knuckles, wrsits, elbows, ankles, knees, and feet.
3.Arthritis affecting the hand joints with at least 1 area swollen in a wrist, knuckle or finger.
4.Symmetric arthritis with simultaneous involvement of the same joint areas on both sides of the body (bilateral involvement of the fingers, knuckles, or feet is acceptable without absolute symmetry.
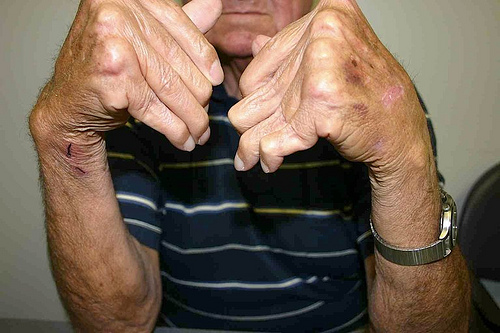
5.Rheumatoid nodules: Subcutaneous nodules over bony prominences, or extensor surfaces, or near joints, observed by a physician.
6.Serum rheumatoid factor: Abnormal amounts of serum rheumatoid factor by any method for which the result has been positive in less than 5 per cent of control subjects.
7.Radiographic (X-ray) changes: Typical of rheumatoid arthritis on x-rays of the hands, wrists. Must include erosions or demineralization in or near involved joints.
For classification purposes, a patient must satisfy at least 4 of the 7 criteria. Criteria 1 through 4 must have been present for at least 6 weeks. Patients with 2 clinical diagnoses are not excluded. While these criteria are fine for standardization purposes when doing research to ensure uniformity, they are not meant to be necessarily followed rigidly in a clinic setting.
More recently, the use of assays such as the anti-cyclic citrullinated peptide (anti-CCP) assay has provided a more specific method for identifying patients whose arthritis symptoms will lead to RA.
In a recent published study, Japanese researchers found that the combination of a positive rheumatoid factor, elevated C-reactive protein, swollen joints, and a positive anti-CCP was highly specific and accurate; it is easy to use for physicians and thus beneficial to patients" (Yamane T, et al. Journal of Rheumatology, January, 2008).
As a practicing rheumatologist, I find this article to be useful in that it confirms what many of us here in the United States have also found to be true. The diagnosis of RA, by all means, is not necessarily easy.
Yet, making the diagnosis is critical to initiating aggressive therapy. What is very important to remember is that today, making the diagnosis of rheumatoid arthritis is not necessarily a bad thing for a patient. Newer biologic drugs have made the "putting a patient into remission" more of a likely scenario than not.
The data from the Japanese study supports a simple yet direct method for making the diagnosis quickly.