Cervical Spondylosis
Cervical spondylosis (spon-dee-low-sis) can be thought of as "grey hair" of the spine. This means that if you live long enough (and that may only mean forty- to fifty-years of age in some populations) x-rays of your spine will eventually show signs of cervical spondylosis.
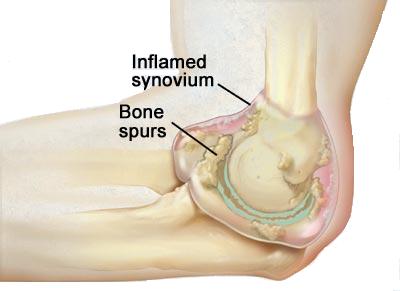
As described above, the term refers to osteophytes (os-t-o-fights), or bony overgrowths, that protrude from the vertebral bodies as well as narrowing occurring across the disc spaces as the disc degenerates. Though they can compress the spinal cord (like Mrs. S) or a spinal nerve root (like Mr. D), the vast majority of these osteophytes do not cause any nerve problems. They are a sign, however, that the disc between the vertebrae and the facets (fah-sets) has become degenerative.
Degenerative discs can cause pain. The mechanism of pain is, unfortunately, not well understood. It is thought to be transmitted by tiny nerve endings that innervate the back part of the disc and facet joints. Degeneration can cause pain from the disc, facet joint, or both concomitantly. Diagnostic efforts are aimed to determine which of these structures are the pain generators. Therapy is directed to relieving stresses being placed on these areas.
Presentation
Mrs. P is a forty-two year old woman who was involved in a motor vehicle accident ten years ago. Since then, her neck has never felt "right." She has frequent neck spasms, which cause her to miss many days of work as an assembly line worker. Mrs. P states her neck pain frequently radiates to the base of her head and down into her shoulder blades. She has no arm or leg pain, no bowel or bladder complaints, and no problems with coordination of her hands or feet.
Mrs. P has taken many pain medications over the past ten years. In the first couple of years, ibuprofen was working adequately. About seven years ago, an emergency room physician gave her a shot of Demerol?, which she felt disagreed with her, but did temporarily relieve her pain. Two weeks later, the pain was back.
Her primary care doctor began to prescribe a mild narcotic, Vicodin?, about three years ago. She takes this on occasion, but she does not like the "spacey" feeling she gets when she takes it. She has had two courses of physical therapy in the past. In describing the therapy she states she was given exercises concentrating on extending her neck. She felt this made her pain worse, despite the therapist's reassurance that this would help relieve the pressure across her intervertebral discs. Mrs. P refuses to go back to physical therapy.
Her primary care doctor has also instructed his patient to use a home traction set up. Attaching to the top of a door, Mrs. P uses upright sitting traction. This consists of a chin-head strap connected to a rope, which runs over a pulley. The other end of the rope has light weights (five to ten pounds) attached, which deliver an upward force along Mrs. P's neck. When she is in the traction setup, she experiences some relief, but it is short-lived. The pain usually returns thirty minutes after she has stopped the traction.
Mrs. P also uses a soft cervical collar when she has extreme neck spasms. Again, the relief is temporary. She returns to her primary care doctor for a regular visit and to discuss the options for her excruciating neck pain.
Examination
Mrs. P's primary care doctor performs a careful neurologic exam, which shows no abnormalities of nerve function. Her neck is stiff with a markedly decreased range of motion. She notices that when the doctor was testing extension (head to the back) the pain became much worse.
Diagnostic Tests
Over the years, Mrs. P has had numerous x-rays of the spine. Her latest x-ray showed degenerative changes with multiple osteophytes growing from the front and back of the C5 and C6 vertebral bodies. An MRI of her neck, taken one year ago, showed no nerve or spinal cord compression, but shortening of the intervertebral disc height. This suggests that the disc has become dried and degenerated and that it is not functioning normally. More importantly, there appears to be degeneration of the facet joints as well at the C5 and C6 level. Having treated Mrs. P's painful neck for many years to no avail, her doctor has decided to seek a specialist consultation from a pain management physician.
Specialist Consultation
The pain management doctor reviews Mrs. P's records, chart, x-rays, and MRI. His examination demonstrates that her pain is worse with extension of the neck. He tells her that she has what appears to be degenerative cervical spondylosis at the C5-6 level. Because her neck pain is worse with extension, the doctor believes that Mrs. P has pain associated with facet arthritis. He suggests that she undergo a series of injections into the facet joints to determine if this decreases her pain. The injections would be Lidocaine? (a numbing medicine) and corticosteroids (to decrease the inflammation). She agrees with this plan.
The injections into the facet joint of C5-6 gave Mrs. P substantial relief. She has seen the pain doctor two more times over the past ten months since her initial visit. Each time, the facet injection helps her pain dramatically to a point where she can skip taking her pain medicines some days. Unfortunately, the effects have lasted only about three months after each injection.
The pain doctor is confident that her "pain generator" is the facet joints at C5-6 in her cervical spine. He explains to Mrs. P that if the pain continues she might be interested in surgery to fuse these two vertebrae together. This would eliminate motion at the painful joints and hopefully relieve her pain. The doctor explains that the procedure has about a 70 percent success rate in providing long-lasting pain relief. He states that he does not perform the surgery and that she would need to be referred to a spine surgeon.
Mrs. P thinks about her options carefully. Though her pain is continuing, she is not willing to have surgery yet. Because of the temporary relief of the injections, she feels that she has been able to resume, to some degree, her regular activities. As this is the first time she has had improvement over the past ten years, she would like to postpone surgery for as long as possible. The doctor agreed fully with this decision. Surgery on the neck for neck pain is not nearly as reliable at relieving pain as is surgery on the neck to decrease arm pain.
Conclusion
Degenerative disorders of the spine continue to be a significant cause of neck pain in today's population. Understanding of these problems continues to grow. With that, patients' understanding should follow suit. Affected patients should be aware of the possible treatment modalities, including medication, therapy, braces, selective injections, and surgery. The best patient is an informed one who understands the natural progression of these disorders, as well as the benefits, risks, and complications of available treatments.
This article is an excerpt from Dr. Stewart G. Eidelson's book, Advanced Technologies to Treat Neck and Back Pain, A Patient's Guide (March 2005).
Copyright © www.orthopaedics.win Bone Health All Rights Reserved