Felty syndrome (FS), which was first described in 1924, is a potentially serious condition that is associated with seropositive (rheumatoid factor [RF]-positive) rheumatoid arthritis (RA).[1] FS is characterized by the triad of RA, splenomegaly, and granulocytopenia. Although many patients with FS are asymptomatic, some develop serious and life-threatening infections secondary to granulocytopenia.
NextAlthough the pathophysiology of FS is not fully understood, evidence points to splenic sequestration and subsequent granulocyte destruction.
Early studies demonstrated that granulocyte counts were lower in the splenic vein than in the splenic artery. Researchers have shown immune complexes coating granulocytes, diminished granulocyte growth factor levels, and numerous circulating autoantibodies, including those against granulocyte surface antigens. T-cell large granular lymphocyte leukemia and FS share overlapping pathophysiologic features.[2]
In a 2002 study from Germany, 15 patients with neutropenia due to FS were matched to a control group of 16 patients with normocytic RA, and 16 patients with neutropenia and systemic lupus erythematosus (SLE) were matched to a control group of 16 patients with SLE.[3] Antibodies against granulocyte colony-stimulating factor (G-CSF) were measured.
In this study, 11 patients with FS demonstrated anti–G-CSF immunoglobulin G (IgG); none of the patients in the RA control group demonstrated anti–G-CSF IgG.[3] In addition, 6 of the patients with both neutropenia and SLE and 6 of the patients in the SLE control group had anti–G-CSF antibodies. These antibodies appeared to have a neutralizing effect on G-CSF.
Risk factors for FS include the following:
FS affects approximately 1-3% of all patients diagnosed with RA, and RA occurs in about 1% of the general population. It appears to be rare in children and the African American population. The true prevalence of FS is difficult to ascertain because many affected patients are asymptomatic. Prevalence may be decreasing with the advent of more potent antirheumatic agents. Few data suggest that the international frequency of FS differs significantly from the US frequency.
FS is most common during the fifth through seventh decades of life and is usually associated with more than 10 years of preceding RA activity. Men are affected with FS earlier in the course of RA than women are. FS is about 3 times more common in females, though underreporting and asymptomatic cases hinder determination of the true sex ratio. FS is most common in whites and is uncommon in blacks. The HLA-DR4 genotype, a marker for more aggressive RA and more frequent extra-articular manifestations in whites, is strongly associated with FS.
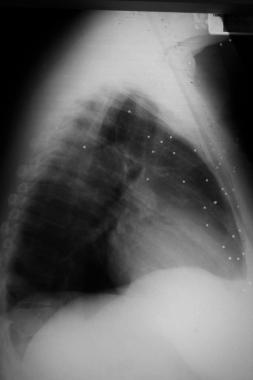
Although many individuals with FS are asymptomatic, others become symptomatic and may develop life-threatening infections. Pulmonary and skin infections are common. Mortality and morbidity are heavily influenced by the level of debilitation due to the underlying RA, along with the extent of immunosuppressive therapy used in treating both RA and FS. One study from southwest England observed 32 patients with Felty syndrome; 5 patients died of overwhelming bronchopneumonia during a mean follow-up period of 5.2 years.[4]
Curiously, over the past 20 years in the United States, the frequency of hospitalization for rheumatoid vasculitis and ultimate splenectomy in patients with FS has dropped, possibly because earlier and more aggressive treatment of RA tends to control the disease before the manifestations of FS appear.
Granulocytopenia is defined as an absolute neutrophil count (ANC) lower than 2000/µL, and the infection risk increases as the ANC drops. Infection incidence increases significantly when the polymorphonuclear leukocyte (PMN) count is lower than 1000/µL.
In a retrospective study of male patients with FS treated at the Department of Veterans Affairs, lymphoproliferative malignancies were more prevalent; in particular, the patients had an increased prevalence of non-Hodgkin lymphoma.[5]
Educate patients with FS about the warning signs of infection and ensure that they have ready access to medical care.
Some practitioners supply FS patients with a broad-spectrum oral antibiotic that is to be taken at the first signs of a bacterial infection. Instruct patients that the decision to initiate antibiotic therapy is a decision that must be made on an individual basis, and advise them to contact their physician immediately if such a situation develops.
Clinical Presentation
Copyright © www.orthopaedics.win Bone Health All Rights Reserved