Radial head fractures and dislocations are traumatic injuries that require adequate treatment to prevent disability from stiffness, deformity, posttraumatic arthritis, nerve damage, or other serious complications. Radial head fractures and dislocations may be isolated just to the radial head (and neck) and the lateral elbow (and proximal forearm), or they may be part of a combined complex fracture injury pattern involving the other structures of the elbow, distal humerus, or forearm and wrist.
Radial head and neck fractures and dislocations have been treated by closed and open methods. Early attempts at closed treatment with casting resulted in stiffness and loss of function in the elbow. Consequently, treatment has evolved so that only patients with fractures stable enough to allow early motion undergo closed treatment, while essentially all other patients are treated with a form of surgical treatment.
Surgical methods have included excision of the fracture fragments, replacement, and internal fixation. Problems with proximal radial migration, especially with excision but also with replacement, and problems with the replacement implants have led to the belief that anatomic reduction and internal fixation is currently the treatment of choice for unstable and displaced radial head and neck fractures and dislocations.[1, 2, 3, 4, 5]
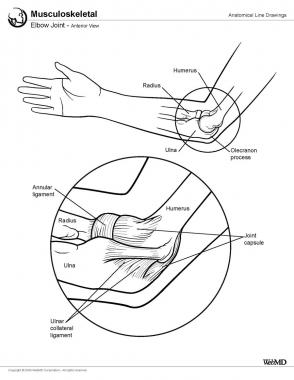
NextThe elbow joint consists of three bones and three joints. The bones are as follows:
The joints are as follows:
The joints are controlled by the ligamentous anatomy of the elbow. The elbow joint (ulnotrochlear joint) is constrained by the medial collateral ligament, which has well-defined anterior, posterior, and transverse bundles. The elbow is also constrained by the lateral collateral ligament, which is poorly defined, and the radial collateral, lateral ulnohumeral, and accessory collateral ligaments provide stability. The radioulnar joint is constrained by the annular ligament.
The neurovascular structures of the elbow are easily damaged in fractures and dislocations of the elbow. The physician needs to be especially aware of the ulnar nerve proximally because it passes behind the medial epicondyle and the posterior interosseous nerve, wraps around the radial neck, and is most likely to be damaged with radial head fractures or dislocations or during surgery to correct these injuries. The median nerve and the brachial artery are in danger in the front of the elbow.
Because the radial head is intra-articular, anatomic reduction of bone fragments is necessary to minimize the risks of lateral posttraumatic arthritis from mechanical grinding. The intra-articular position also means that soft-tissue attachments to the most proximal portion of the bone are limited, and thus, fractured fragments frequently lose their blood supply, resulting in avascular necrosis and potential nonunion. Luckily, the radial head mostly acts as a spacer preventing proximal migration of the radius; as long as it maintains its structural support, the patient may do well even if the bone dies.
Except for congenital radial head dislocations, which by definition are not acquired, radial head fractures and dislocations are the result of trauma, usually from a fall on the outstretched arm with the force of impact transmitted up the hand through the wrist and forearm to the radial head, which is forced into the capitellum.
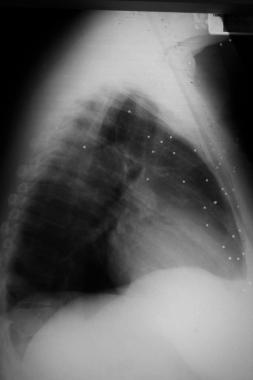
Recognizing a congenital radial head dislocation (see the image below), in which the radial head is larger and rounder than expected, is important because operative treatment to reduce a congenital radial head dislocation is not indicated.
 Congenital radial head dislocation.
Congenital radial head dislocation.
The radial head is fractured in about 20% of cases of elbow trauma. About 33% of elbow fractures and dislocations include injury to the radial head, the radial neck, or both.
For radial head and neck fractures and dislocations, the prognosis is generally good when the following are achieved[6] :
A study by Duckworth et al reported excellent long-term results with nonoperative management of isolated stable fractures of the radial head or neck.[7]
Clinical Presentation
Copyright © www.orthopaedics.win Bone Health All Rights Reserved