Normal positioning and movement of the digits depends on the functional integrity of extrinsic and intrinsic muscles. The extrinsic muscles originate in the forearm, and the intrinsic muscles originate distal to the wrist. The intrinsic muscles are traditionally divided into 5 groups: thenar, hypothenar, palmar interossei,[1] dorsal interossei, and lumbricals.
The 4 thenar muscles are the abductor pollicis brevis, flexor pollicis brevis, opponens pollicis, and adductor pollicis. The abductor pollicis brevis abducts the thumb away from the palm. The flexor pollicis brevis flexes the thumb metacarpophalangeal (MCP) joint. The opponens pollicis abducts, flexes, and pronates the first metacarpal. With these muscles, the thumb is brought from lateral to medial position across the palm in opposition to the 4 ulnar digits. The adductor pollicis adducts the thumb toward the palm.
The hypothenar muscles are the abductor digiti minimi, the flexor digiti minimi brevis, and the opponens digiti minimi. The abductor digiti minimi abducts the little finger away from the fourth finger. The flexor digiti minimi brevis flexes the little finger at the MCP joint. The opponens digiti minimi abducts, flexes, and supinates the fifth metacarpal. With these muscles, the little finger is brought into opposition to the thumb.
Most anatomists describe 3 palmar interossei and 4 dorsal interossei muscles. The dorsal interosseous muscles flex the MCP joints and extend the interphalangeal (IP) joints. The dorsal interossei also abduct the 4 ulnar digits from one another; the volar interosseous muscles adduct the 4 ulnar digits together toward the third finger. There are 4 lumbrical muscles. They function as a connection between the flexor digitorum profundus (FDP) and the extensor mechanism. Their main function is to facilitate extension of the IP joints. The lumbricals can extend the IP joints in any position of the MCP joints.
An image depicting the Froment sign can be seen below.
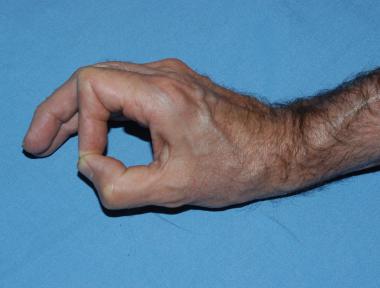 Image in a patient with ulnar neuropathy demonstrates the Froment sign during pinching. Loss of the ulnar-innervated adductor pollicis results in reliance on the flexor pollicis longus and exaggerated interphalangeal (IP) joint flexion. Loss of the metacarpophalangeal (MCP) joint flexor leads to MCP hyperextension over time.
Image in a patient with ulnar neuropathy demonstrates the Froment sign during pinching. Loss of the ulnar-innervated adductor pollicis results in reliance on the flexor pollicis longus and exaggerated interphalangeal (IP) joint flexion. Loss of the metacarpophalangeal (MCP) joint flexor leads to MCP hyperextension over time.
The ulnar nerve innervates most of the intrinsic muscles in the hand: all the interossei, the 3 hypothenar muscles, the adductor pollicis, the deep head of flexor pollicis brevis, and the 2 ulnar lumbricals. All remaining intrinsic muscles—that is, the 2 radial lumbricals, the abductor pollicis brevis, the opponens pollicis, and the superficial head of the flexor pollicis brevis—are thus innervated by the median nerve.[2]
Table. Muscles of the Forearm (Open Table in a new window)
Muscles of anterior fascial compartment Name of Muscle Nerve Supply Pronator teres Median nerve Flexor carpi radialis Median nerve Palmaris longus Median nerve Flexor carpi ulnaris Ulnar nerve Flexor digitorum superficialis Median nerve Flexor pollicis longus Anterior interosseousMedian nerve injuries are commonly referred to as high (ie, at or above the elbow) or low (ie, distal to mid forearm). While a high injury affects both intrinsic and intrinsic motor function, a low injury affects only intrinsic motor function.
A high median nerve division paralyzes the extrinsic muscles: pronator teres, flexor carpi radialis, palmaris longus, flexor digitorum superficialis (FDS), flexor pollicis longus, radial half of the FDP, and pronator quadratus. As a result, the forearm tends to rest in supination with the wrist in ulnar deviation. The median-innervated intrinsic muscles are also paralyzed. The lumbricals to the index and long fingers are paralyzed. Therefore, only weak flexion of the MCP joints is possible with the ulnar-innervated interosseous muscles.[3, 4, 5]
The IP joints of the thumb and the index and middle fingers cannot flex as a result of paralysis of the FDP and FDS motor units. If the ulnar nerve supplies the FDP to the ring finger, the ring finger IP joints can then flex. The ulnar nerve supplies the FDP motor units to the ring and little fingers, so the fourth and fifth fingers can flex. The abductor pollicis brevis, and opponens pollicis muscles are paralyzed. The thumb rests in the plane of the palm and cannot be positioned for a pulp-to-pulp pinch between the thumb and fingers. The thumb IP joint is extended due to paralysis of the flexor pollicis longus.
Median nerve injury at the wrist preserves extrinsic muscle function. The pronator teres, FDS, FDP, and flexor pollicis longus motor units are intact. The first 2 lumbricals, the abductor pollicis brevis, and the opponens pollicis are paralyzed. When the patient slowly makes a fist, the index and middle fingers clearly lag behind the fourth and fifth fingers because of a lack of initiation of flexion at the MCP joints by the lumbricals. The thumb rests in the plane of the palm and cannot oppose the fingers (see image below). The patient can flex the thumb terminal phalanx because the flexor pollicis longus is not paralyzed.
 The intrinsic muscles innervated by the median nerve (abductor pollicis brevis and opponens pollicis) are checked by resisting palmar abduction of the thumb.
The intrinsic muscles innervated by the median nerve (abductor pollicis brevis and opponens pollicis) are checked by resisting palmar abduction of the thumb.
Ulnar nerve lacerations are commonly referred to as high or low to reflect whether the injury affects extrinsic and intrinsic muscles.[4, 6, 7, 8]
High ulnar nerve injury results in paralysis of the flexor carpi ulnaris and the ulnar half of the flexor FDP muscles, generally FDP III-V. The distal phalanges of the fourth and fifth fingers cannot flex. Because the FDP motor units have a common origin, some weak flexion of the fourth and fifth fingers may be possible, even if the ulnar half is supplied by the ulnar nerve. An attempt to flex the wrist results in radial deviation due to paralysis of the flexor carpi ulnaris.
All 7 interosseous muscles, the third and fourth lumbrical muscles, the adductor pollicis muscle, generally also one head of FPB, and all 3 hypothenar muscles (flexor digiti minimi brevis, abductor digiti minimi, and opponens digiti minimi) are paralyzed. The patient cannot adduct or abduct the fingers. If the examiner places a piece of paper between the patient's fingers he or she cannot hold it when the examiner pulls the paper away.
The MCP joints are hyperextended, and the IP joints are flexed. These changes are more obvious at the ring and little fingers, because the first and second lumbrical muscles are not paralyzed. This condition is called a claw-hand deformity . The thumb can weakly adduct through the extensor pollicis longus. The patient can pinch and hold a paper between the thumb and index finger by strongly flexing the IP joint with the flexor pollicis longus. The combination of strong IP and weak MCP flexion called the Froment sign.
Ulnar nerve injury at the wrist spares the flexor carpi ulnaris and the medial half of the FDP muscles. The patient can flex the wrist and all the distal IP (DIP) joints. However, all intrinsic muscles innervated by the ulnar nerve are paralyzed, and both the clawhand deformity and the Froment sign are prominent (see image below).
Image in a patient with ulnar neuropathy demonstrates the Froment sign during pinching. Loss of the ulnar-innervated adductor pollicis results in reliance on the flexor pollicis longus and exaggerated interphalangeal (IP) joint flexion. Loss of the metacarpophalangeal (MCP) joint flexor leads to MCP hyperextension over time.
Next
Open or closed trauma is the most frequent cause of intrinsic hand deformities. Although sensory loss contributes to the overall impairment, it does not contribute to the deformity. Ulnar nerve compression can occur at the elbow (the cubital tunnel) or at the wrist (in the Guyon canal). Median nerve compression associated with intrinsic loss can occur with pronator syndrome or carpal tunnel syndrome. Anterior interosseous nerve compression does not result in intrinsic loss because this nerve innervates only the extrinsic motor units.
One third of all patients with rheumatoid disease (RA) develop some degree of intrinsic contracture during the course of their disease, Hand deformities tend to progress in RA.[9] Peripheral nerve palsy, most commonly afflicting the ulnar nerve at the elbow, occurs in 20-25% of patients with leprosy. Claw hand due to ulnar nerve paresis is therefore the most common presentation in this group of patients.
Intrinsic muscle contracture can be caused by trauma,[10] inflammation, tumor, central nervous system disease, joint destruction, leprosy (Hansen disease), compartment syndrome, or rheumatoid disease.
Fixed contractures of the intrinsic muscles may severely impair the function of the hand. A mild contracture may inhibit certain hand functions without any gross deformity. The patient may complain of a weak grip when using, for example, a screwdriver or a hammer. Severe contractures cause MCP joint flexion and IP joint extension, resulting in an intrinsic-plus deformity. The patient experiences difficulty in grasping, pinching, and abducting the fingers. In combination with sensory loss, the hand is severely disabled.
Individual involvement of intrinsic muscles results in characteristic deformities. Lumbrical contracture causes finger extension while the patient is trying to flex the finger. The origin of the lumbrical is pulled proximally with extrinsic flexion, and the IP joints are extended.
Contraction of the abductor digiti minimi presents as small-finger abduction and causes MCP joint flexion and IP joint extension. Thenar intrinsic muscle contracture can cause thumb adduction, MCP joint flexion, and IP joint hyperextension. The patient loses effective pinch, large-volume grip, and hand dexterity.
The patient may present with a history of trauma, inflammation, tumor, leprosy disease, compartment syndrome, or rheumatoid disease.
The first dorsal interosseous muscle is tested by having the patient place the ulnar side of the hand on the examination table. The radial side of the index finger is facing up. The patient is asked to raise the index finger toward the ceiling. The examiner applies resistance and observes the patient's strength. Muscle strength testing is likely to be more sensitive if the right and left sides are tested simultaneously rather than one after the other.[11]
The second, third, and fourth dorsal interosseous muscles are tested by having the patient place the palm on the examination table. The patient spreads all of the fingers against resistance (see image below). The volar interosseous muscles are examined by placing a piece of paper between the digits and by having the patient hold his or her fingers tightly together as the examiner tries to withdraw the paper. The test is repeated between each of the adjacent fingers.
 The ulnar-innervated intrinsic muscles can be checked by resisting abduction of the index (first dorsal interosseous muscle) and small fingers (abductor digiti quinti muscle).
The ulnar-innervated intrinsic muscles can be checked by resisting abduction of the index (first dorsal interosseous muscle) and small fingers (abductor digiti quinti muscle).
Adhesions and contractures of the intrinsic and extrinsic extensor muscles can limit flexion of the digits. The intrinsic tightness test can be used to differentiate extrinsic pathology from intrinsic pathology. During a test for intrinsic tightness, the examiner usually attempts to fully flex the proximal interphalangeal (PIP) joint of an examined finger while the MCP joint is kept in full extension and flexion, respectively. In the case of intrinsic tightness, (passive) flexion of the IP joint is more restricted when the MCP joint is in extension than when the MCP joint is in flexion (see image below).
 The gloved examiner checks for intrinsic tightness. With the metacarpophalangeal (MCP) joint hyperextended, the proximal interphalangeal (PIP) joint is passively flexed. The intrinsic muscles are volar to the axis of rotation of the MCP joint and dorsal to the axis of the PIP joint. MCP joint hyperextension tightens the intrinsics. Results of this test are compared with those in the contralateral, normal hand. Note intrinsic atrophy in the first dorsal web space.
The gloved examiner checks for intrinsic tightness. With the metacarpophalangeal (MCP) joint hyperextended, the proximal interphalangeal (PIP) joint is passively flexed. The intrinsic muscles are volar to the axis of rotation of the MCP joint and dorsal to the axis of the PIP joint. MCP joint hyperextension tightens the intrinsics. Results of this test are compared with those in the contralateral, normal hand. Note intrinsic atrophy in the first dorsal web space.
If the intrinsic muscles are scarred, passive MCP joint extension increases PIP joint extension and makes passive PIP joint flexion more difficult (see images below).
 Image in a patient with a partial ulnar nerve paralysis is asked to extend the digits. Hyperextension of the metacarpophalangeal (MCP) joints of the ring and small fingers occurs with the loss of intrinsic ulnar-innervated MCP flexors. The index and middle fingers have median innervated intrinsics (lumbricals) that allow the extrinsics to extend the interphalangeal (IP) joints.
Image in a patient with a partial ulnar nerve paralysis is asked to extend the digits. Hyperextension of the metacarpophalangeal (MCP) joints of the ring and small fingers occurs with the loss of intrinsic ulnar-innervated MCP flexors. The index and middle fingers have median innervated intrinsics (lumbricals) that allow the extrinsics to extend the interphalangeal (IP) joints.
 When the examiner prevents metacarpophalangeal hyperextension of the ring and fifth fingers, the patient can completely extend the interphalangeal joints with the extrinsic tendons.
When the examiner prevents metacarpophalangeal hyperextension of the ring and fifth fingers, the patient can completely extend the interphalangeal joints with the extrinsic tendons.
The abductor pollicis brevis is tested as the patient pushes against resistance while the thumb is in the abducted position. The opponens pollicis is similarly tested with the thumb more circumducted. The adductor pollicis is evaluated as the patient pinches a piece of paper between the thumb and index finger while the examiner pulls on the paper. The flexor pollicis brevis is assessed with the thumb MCP joint in flexion and with resistance applied volarly.
The abductor digiti minimi is tested by having the patient place the back of the hand on the examining table while the little finger is abducted against resistance. The flexor digiti quinti is examined by flexing the MCP joint while the finger is adducted. The IP joints must be kept in extension. To test the opponens digiti minimi, the patient performs a pulp-to-pulp pinch by moving the little finger to the thumb.
Intrinsic tightness can result in a swan-neck deformity, which is characterized by PIP joint hyperextension and DIP joint flexion. The tight intrinsic muscles pull the PIP joints into extension, which allows passive DIP joint flexion. Over time, the PIP joint volar plate stretches as the extensor mechanism pulls the proximal phalanx into hyperextension. As PIP joint hyperextension increases, DIP joint flexion increases.
Intrinsic contracture disturbs fine hand-muscle balance. The fingers become stiff, function deteriorates, and the hand becomes disabled.
The boutonniere deformity involves PIP joint flexion and hyperextension of DIP and MP joints. Attenuation of the central slip with separation from the transverse retinacular ligaments cause migration of the lateral bands volar to the PIP joint rotational axis. Thus the lateral bands act as flexors of the PIP joint. As a result, the FDS meets less resistance and flexes the PIP joint. Contraction of the lateral bands and oblique retinacular ligaments prevents extension of the PIP joint. The lateral bands extend the DIP joint. The MCP joint hyperextends as the sagittal band applies traction on the extensor tendon.[12, 13, 14]
Physical examination involves evaluation of the range of motion, both active and passive, of both DIP and PIP joints. The examiner tries to passively flex the DIP joint while passively extending the PIP joint. In the presence of boutonniere deformity, both lateral bands and oblique retinacular ligaments are contracted and the DIP joint will not flex. The examiner flexes the PIP joint, and the DIP joint can then actively and passively flex because both the lateral bands and the oblique retinacular ligaments are now relaxed.
Intrinsic and extrinsic tightness may coexist in the same patient. Intrinsic contracture may not be clinically apparent until associated extrinsic changes are corrected.
In cases of extrinsic tightness, PIP joint flexion increases when the MCP joint is extended and decreases when the MCP joint is flexed.
Workup
Copyright © www.orthopaedics.win Bone Health All Rights Reserved