Mononeuropathies are a form of peripheral neuropathy characterized by sensory disturbances and/or motor deficits in the distribution of the affected nerve. They can occur secondary to direct trauma, compression, stretch injury, ischemia, infection, or inflammatory disease. In the lower extremity, peroneal neuropathy is the most common isolated mononeuropathy and the third most common mononeuropathy overall. Peroneal mononeuropathy may result in the clinical complaint of pain and sensory disturbances in the lateral lower limb and dorsal foot, and weakness of the ankle dorsiflexors and evertors. The peroneal nerve is also known as the superficial peroneal nerve and more recently the superficial fibular nerve.[1]
NextCompression and entrapment neuropathies are predominantly demyelinating.
The pathophysiology of ischemic injuries and nerve transection is axonal damage. When axonal damage occurs, recovery is slower and longer and may not be complete.
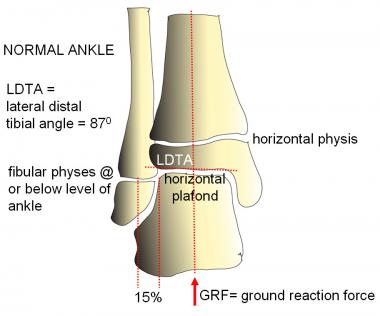
Knowledge of peroneal nerve anatomy is essential to understanding the mechanism of its injury and to localizing the site of the lesion.[2]
No racial predilection is known.
No gender proclivity is known.
Peroneal mononeuropathy is uncommon in children but has been reported in all age groups.
Dancers are also prone to superficial and deep peroneal nerve entrapments.[3]
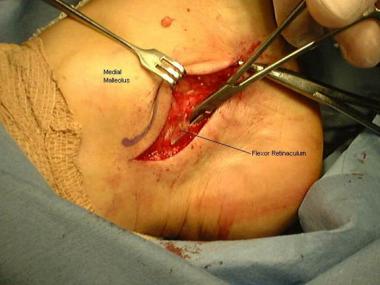
Common peroneal nerve decompression is a useful procedure to improve sensation and strength as well as to decrease pain.[4]
A retrospective study evaluated electrodiagnostic prognostic factors after peroneal nerve injury in 39 subjects. Outcome was associated with compound muscle action potential responses from extensor digitorum brevis and tibialis anterior: 81% of subjects with any tibialis anterior response and 94% with any extensor digitorum brevis response had a good outcome (at least 4 of 5 ankle dorsiflexion strength) compared with those with absent responses (46% and 52%, respectively). In addition, all patients with nontraumatic compression had a good outcome.[5]
Clinical Presentation
Copyright © www.orthopaedics.win Bone Health All Rights Reserved