Hammertoe deformity is the most common deformity of the lesser toes. The fundamental problem is a chronic, sustained imbalance between flexion and extension force of the lesser toes from intrinsic forces, extrinsic forces, or both.
With progressive proximal interphalangeal (PIP) joint flexion deformity, compensatory hyperextension of the metatarsophalangeal (MTP) and distal interphalangeal (DIP) joints typically occurs. The hyperextension of the MTP joint and the flexion of the PIP joint make the PIP joint prominent dorsally. This prominence rubs against the patient's shoe, causing pain.
Early in its natural history, the deformity is flexible and passively correctable, but with time, it typically becomes fixed. Progressive deformity can lead to MTP joint dislocation. Once flexion contractions form, surgical treatment may be indicated. Surgical treatment of hammertoe deformity has historically been based on altering the relative lengths of the toe and its tendons in order to achieve balance between extensor and flexor forces. Options have included the following:
Metatarsal shortening has gained renewed interest, but PIP joint resection arthroplasty and tendon transfers are the main procedures for hammertoe correction.
NextThe lesser toe comprises three phalanges that articulate at the PIP and DIP joints. The proximal phalanx articulates with the metatarsal at the MTP joint. Medial and lateral collateral ligaments, a fibrocartilaginous plantar plate, and a thin dorsal capsule stabilize each of the three joints.
The extensor digitorum longus (EDL) tendon originates in the leg and crosses the ankle anteriorly. Although it extends all three joints of the lesser toe, it primarily acts at the MTP joint. The extensor digitorum brevis (EDB) originates in the sinus tarsi and blends with the EDL tendon over the proximal phalanx to form the extensor expansion. The EDL continues distally from the extensor expansion and trifurcates to form the central slip, which inserts onto the middle phalanx, and the lateral bands, which insert onto the distal phalanx. The central slip and lateral bands extend the PIP and DIP joints, respectively, when the MTP joint is in neutral position or in plantarflexion.
The flexor digitorum longus (FDL) tendon originates in the leg, crosses the ankle medially, and flexes all three joints of the lesser toes, though it acts primarily at the DIP joint. The flexor digitorum brevis (FDB) tendon originates from the plantar surface of the calcaneus and primarily flexes the PIP joint. The lumbricals originate from the medial and lateral surfaces of the metatarsals, pass plantarly to the MTP, and then extend dorsally to coalesce with the lateral bands. Thus, the lumbricals flex the MTP joint and extend the PIP and DIP joints.
The neurovascular bundles of each toe arise from a common interdigital artery and a common interdigital nerve. Each bifurcates at approximately the level of the MTP joint. Each branch then extends along the medial and lateral aspects of the toe deep to the subcutaneous tissue. Both the interdigital artery andthe interdigital nerve are plantar to the intermetatarsal ligament at the level of the MTP joint. Both can become contracted in a chronic hammertoe and are subject to traction injury with hammertoe correction.
The fundamental problem is a chronic, sustained imbalance between flexion and extension force of the lesser toes from intrinsic forces, extrinsic forces, or both. Hammertoe deformity primarily comprises flexion deformity of the PIP joint of the toe, with hyperextension of the MTP and DIP joints (see the image below).
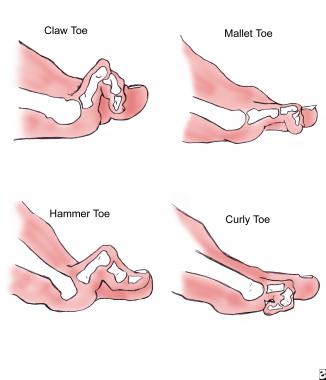 Diagram comparing clinical appearances of lesser-toe deformities.
Diagram comparing clinical appearances of lesser-toe deformities.
When a foot's second ray is longer than the first and shoe wear does not fit correctly, flexion of the PIP joint occurs to accommodate the shoe. This length difference also causes MTP synovitis to develop from overuse of the second MTP joint. Attenuation of the collateral ligaments and plantar plate results, and the MTP joint hyperextends and may even progress to dorsal subluxation or dislocation (see the image below). Rheumatoid arthritis causes hammertoe deformity by progressive MTP joint destruction, leading to MTP joint subluxation and dislocation.[1, 2, 3]
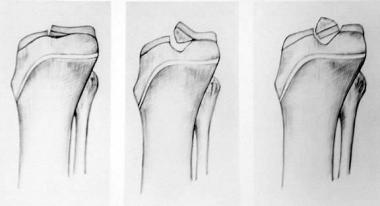
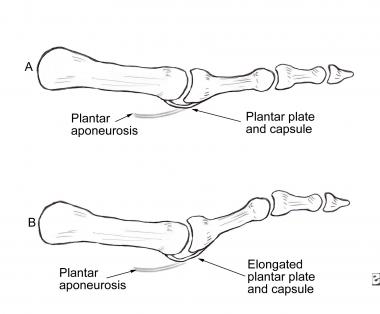 Pathomechanics of hammertoe deformity. Elongated plantar plate, caused by either metatarsophalangeal (MTP) synovitis and instability or chronic MTP hyperextension due to toe crowding, results in MTP subluxation or dislocation with compensatory proximal interphalangeal (PIP) flexion.
Pathomechanics of hammertoe deformity. Elongated plantar plate, caused by either metatarsophalangeal (MTP) synovitis and instability or chronic MTP hyperextension due to toe crowding, results in MTP subluxation or dislocation with compensatory proximal interphalangeal (PIP) flexion.
With all three of these etiologies, the EDL tendon gradually loses mechanical advantage at the PIP joint, as does the FDL tendon at the MTP joint. The intrinsic muscles sublux dorsally as the MTP hyperextends. They now extend the MTP joint and flex the PIP joint, as opposed to their usual functions of flexing the MTP joint and extending the PIP joint.
Etiologies of hammertoe deformity include the following:
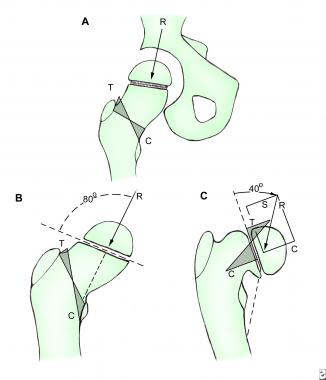
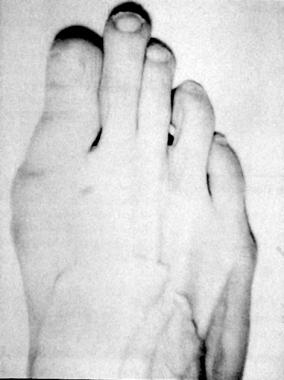 Morton foot, wherein second ray (metatarsal and corresponding toe) is longer than first ray.
Morton foot, wherein second ray (metatarsal and corresponding toe) is longer than first ray.
MTP synovitis and instability are associated with a second ray that is longer than the first. Inflammatory arthropathies typically involve more than one of the lesser MTP joints. Ill-fitting shoe wear compounds the effects of any of the other causes.
The incidence of hammertoe deformity is undefined. However, the condition is strongly associated with the presence of a second ray that is longer than the first, and it is known to be more common in women and to increase in frequency with advancing age. Indeed, this length disparity is found in most patients presenting with foot complaints, though the actual prevalence of this foot shape also is undefined.
Patients should be counseled that their expectations for a good result after hammertoe treatment should include the following:
Although nonoperative treatment of hammertoe deformity often successfully alleviates pain, the deformity typically progresses in magnitude and stiffness in most cases despite diligent nonoperative care. Surgical treatment of flexible hammertoe deformity reliably corrects the deformity and alleviates pain. Recurrence and progression are common, especially if the patient resumes wearing deforming shoes. Surgical treatment of fixed hammertoe deformity provides very reliable deformity correction and pain relief. Recurrence is rare after appropriate surgical management.
Clinical Presentation
Copyright © www.orthopaedics.win Bone Health All Rights Reserved