Ankle dislocations without fracture occur when significant force applied to the joint results in loss of opposition of the articular surfaces. Because of the large amount of force required and the inherent stability of the tibiotalar joint, dislocation of the ankle joint is rarely seen without an associated fracture. Certain researchers argue this is due in part to the strength of the ankle joint ligaments and the relative weakness of the bones that make up the ankle.[1]
A paucity in the medical literature exists illustrating critical examination of the injury, treatment protocol, and outcomes. In 1939, Wilson, Michele, and Jacobsen discussed ankle dislocations without fracture but were limited to 2 private patient case studies and only 14 cases that had been previously reported since 1913.[2] It was this study that attempted a literature review, evaluation of the mechanism, treatment, and results. Again, in 1991, further lack of ankle dislocation research prompted Moehring et al to compile one of the larger series of open ankle dislocation.[3] Recently, most literature demonstrates isolated cases studies of pediatric and adult tibiotalar/ankle dislocations.
Some controversy exists regarding the treatment of ankle dislocations. However, the outcomes appear to be satisfactory in cases treated with immediate reduction of the joint and relief of neurovascular stress as the primary goals of treatment.[4]
Karampinas et al performed a retrospective evaluation of complete talar extrusion without associated fractures and immediate reimplantation and reported that it is important to attempt reimplantation of the talus because of good final outcomes. According to the authors, even in the case of a catastrophic complication, this technique ensures adequate bone stock for additional surgical procedures. The dislocated talus was reduced and held in place with 2 Steinmann pins placed from the inferior aspect of the calcaneus, through the talus, and into the inferior aspect of the tibia. An external fixator was used to stabilize the limb.[5]
NextThe ankle joint is designed for a balance of stability and flexibility, particularly the former. Joint stability is provided by close articulation of the talus with the tibia and fibula. The mortise design further enhances the stability of the configuration.
The talus is trapezoidal in shape, with the greater width anteriorly and narrower posteriorly. As the joint moves into plantar flexion, the talus becomes narrower, resulting in a decrease in stability. It is important to note that this position of plantar flexion is typically in conjunction with the foot being in a supinated position. Thus, despite the foot, particularly the subtalar joint, being in a stable position with all the lesser tarsal bones stacked upon each other, the ankle remains vulnerable to inversion strain and subsequent injury. Conversely, the dorsiflexion of the talus in the ankle joint is typically accompanied by a foot being in the pronated position. Although inversion stress is greatly reduced, strain upon the syndesmotic ligament, medial malleolus, and medial deltoid ligament structures are their greatest disadvantage.[6, 7]
During normal walking, the ankle joint bears 3-5 times the body's weight. This factor increases several fold during running and jumping activities. As weight is applied on heel strike, the fibula descends to increase stability of the ankle joint.
See the image below.
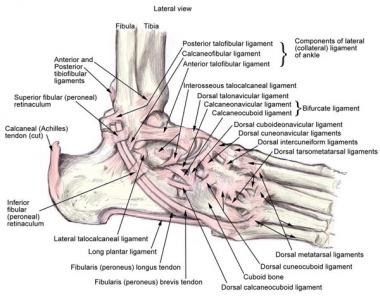 Anatomy of the lateral ankle ligamentous complex and related structures.
Anatomy of the lateral ankle ligamentous complex and related structures.
Associated fractures are the rule rather than the exception with ankle dislocations. Ligamentous disruption varies according to the type of dislocation. (See Ankle Injury, Soft Tissue.) Neurovascular injury is the principal concern, as with any dislocation. Vascular compromise may result in avascular compromise of the talus, permanent sensation or nerve damage, and lower extremity tissue necrosis; and gangrene may occur if not promptly reduced. Tented skin may be subject to ischemic necrosis
Children and adolescents have the most ankle dislocations. Dislocations of the ankle are seen more frequently in young males than in any other group. This presumably is related to their increased risk overall for traumatic injury.
Postmenopausal women are at higher risk for associated fractures. Increased fracture risk probably is related to osteoporotic changes in this subset of patients.
Dislocated ankles should not be expected to return to premorbid function.
The amount of force and level of capsular disruption required to dislocate the inherently stable joint results in significant injury with lasting effects. To a limited extent, prompt intervention can reduce the risk of complications.
For patient education resources, see the Breaks, Fractures, and Dislocations Center, as well as Ankle Fracture.
Clinical Presentation
Copyright © www.orthopaedics.win Bone Health All Rights Reserved